Maslow’s Hierarchy of Needs
Key Points
- Maslow’s model prioritizes human needs from physiologic survival to self-actualization.
- Residents often cannot engage higher-level goals when basic comfort and safety are unmet.
- Physiologic need stabilization is the foundation that enables higher-level need progression in later-life care.
- Nursing priorities in practice map first to physiologic and safety needs.
- When many cues are present, ABCs and Maslow filtering helps identify which findings need immediate action.
- Need levels are fluid and can require concurrent support rather than strict one-way progression.
- In clinical prioritization, safety/security needs are tightly linked to lower-tier physiologic stability.
- Chronic maladaptive stress can disrupt needs across all five levels, not only physiologic stability.
Pathophysiology
Maslow’s hierarchy is a motivation and behavior framework rather than a disease mechanism. In nursing care, it functions as a practical model for prioritizing interventions when multiple needs compete.
The five levels include physiologic needs, safety, love and belonging, esteem, and self-actualization. Maslow proposed that persistent deficits in lower levels can limit engagement in higher-level psychosocial growth.
Maslow also described relative rather than absolute fulfillment: needs can be partially met at multiple levels at the same time, with higher-level fulfillment typically less complete than lower-level fulfillment. Later interpretations added self-transcendence as striving for meaning beyond self-interest, which may appear in care decisions involving sacrifice, legacy, spirituality, or service.
In stress-adaptation care, long-term unresolved stress can progressively erode each level (physiologic function, security, belonging, esteem, and self-actualization), especially when chronic illness and social strain coexist.
For nursing assistants, this model supports holistic care by integrating basic physical needs with emotional security, social connection, and meaning-making.
Classification
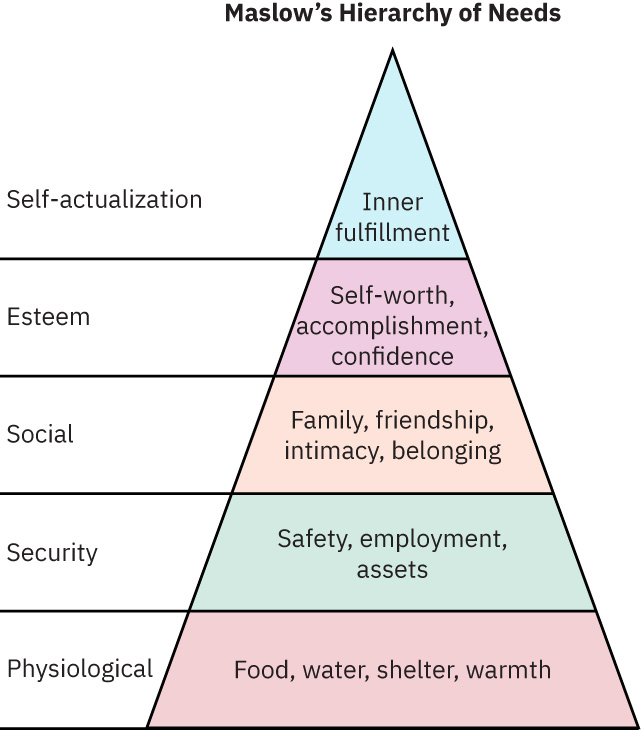 Illustration reference: OpenStax Fundamentals of Nursing Ch.4.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.4.2.
- Physiologic needs: Air, food, hydration, sleep, warmth, pain relief, glucose stability, and other survival fundamentals.
- Safety needs: Predictability, freedom from harm, fall prevention, and physical-psychological security.
- Love and belonging: Connectedness with family, peers, and supportive communities.
- Esteem needs: Respect, dignity, self-worth, and sense of contribution.
- Self-actualization: Personal fulfillment, purpose, and reaching individual potential.
- Self-transcendence (extended model): Meaning and purpose directed beyond oneself.
- Stress-impact mapping: Physiologic instability, safety/resource disruption, social isolation, self-worth erosion, and blocked higher-level fulfillment.
Nursing Assessment
NCLEX Focus
Priority questions often ask which unmet basic need should be addressed before psychosocial goals.
- Assess whether immediate physiologic concerns are preventing participation in other care goals.
- Assess whether chronic stress effects are disrupting multiple need levels simultaneously (for example health decline with resource insecurity and social withdrawal).
- Identify safety threats such as fall risk, unfamiliar surroundings, or fear-related behaviors.
- Evaluate social isolation, loss of belonging, and barriers to meaningful relationships.
- Observe cues of reduced self-esteem, including withdrawal, hopeless statements, or loss of interest.
- Differentiate physical care needs from physiologic-function concerns because both may require separate interventions.
Nursing Interventions
- Follow the care plan to stabilize basic comfort and physiologic needs first.
- In competing-need situations, resolve life-preserving physiologic threats before psychosocial goals.
- When chronic stress is present, use level-by-level prioritization (physiologic to self-actualization) to set realistic staged goals.
- Implement and maintain safety precautions, including fall-prevention strategies.
- Use level-linked nursing actions in older-adult care (for example ADL/hydration/medication support, fall prevention, depression screening, social-family-spiritual connection, dignity-preserving independence coaching).
- Provide prompt responses and a calm routine to improve predictability and trust.
- Respect preferences in grooming, bathing, meals, and personal belongings to support dignity.
- Encourage social engagement and facilitate access to spiritual or community resources when desired.
- Support self-actualization goals when basic needs are stabilized, including meaning-focused planning in serious illness.
Misaligned Prioritization
Pushing higher-level activities before basic comfort and safety are addressed can increase anxiety, refusal of care, and poor outcomes.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| anxiolytics | PRN anxiety agents | Medication support does not replace correction of unmet basic and safety needs. |
| sleep aids | Nighttime sedative-hypnotics | Reassess sleep environment, pain, and comfort factors before escalating pharmacologic support. |
Clinical Judgment Application
Clinical Scenario
A newly admitted long-term care resident repeatedly declines group activities and becomes agitated during evening care.
- Recognize Cues: New environment, fear, poor sleep, and refusal behavior.
- Analyze Cues: Safety and physiologic comfort needs are likely not yet stabilized.
- Prioritize Hypotheses: Immediate priority is reducing insecurity and meeting basic needs.
- Generate Solutions: Establish routine, improve comfort, respond quickly to call light, and introduce social support gradually.
- Take Action: Coordinate care timing and communicate observations to the nurse.
- Evaluate Outcomes: Resident anxiety decreases and participation in care improves.
Related Concepts
- fall-prevention - Safety-level interventions protect residents from injury.
- communication-process - Therapeutic communication helps identify unmet needs.
- caring-for-clients-with-dementia - Behavioral cues often reflect unmet comfort or security needs.
- psychosocial-adaptation-to-parenthood - Developmental transitions reshape belonging and esteem needs.
- nursing-process - Structured assessment helps prioritize needs logically.
Self-Check
- Which unmet need level should be addressed first when a resident is anxious and refusing care?
- How can CNA routines increase a new resident’s sense of safety?
- Which interventions support belonging and esteem without ignoring physiologic priorities?