Healthcare Delivery Models and Organizational Structures
Key Points
- Health systems differ by financing model, governance, and service organization.
- Common model categories include Beveridge, Bismarck, National Health Insurance, and Out-of-Pocket structures.
- U.S. health care is a hybrid that combines elements of all four major model archetypes.
- U.S. delivery includes for-profit, not-for-profit, and government institutions across public and private sectors.
- Integrated delivery systems improve continuity by linking services and information across care settings.
- Delivery settings span inpatient, subacute, outpatient, post-acute, and community adult-care services, each with different goals and staffing intensity.
- Organization type changes tax, profit, charity-care, and safety-net obligations that directly affect access pathways.
- U.S. health spending can rise while outcomes lag peer nations, so financing decisions must be judged by value, not spending volume alone.
- Diffusion of new medical technology can be a major expenditure driver, so adoption decisions should use explicit cost-effectiveness and equity criteria.
- The ACA (signed in March 2010) expanded coverage with stronger preexisting-condition protections and broader essential-benefit access.
- ACA-era protections improved fairness, but affordability pressure (premiums, out-of-pocket costs, and formulary limits) still affects real access.
- U.S. funding streams combine government programs, employer/Marketplace private insurance, and self-pay pathways that create different access constraints.
- Demographic shifts (aging population, increasing diversity, and immigration-driven growth) continuously reshape service demand and delivery priorities.
- Public-health policy delivery uses mechanism categories such as fiscal policy, regulation, education, preventive treatment, and screening.
- Pharmaceutical affordability and access are shaped by global supply-chain resilience, PBM pricing intermediaries, and policy levers such as Medicare inflation-rebate requirements.
- Laws and policies interact but are not interchangeable: laws are government-enforced rules, while policies are structured action frameworks used by governments, professions, and institutions.
Pathophysiology
This concept describes macro-level health system design rather than disease physiology. System structure influences access, coordination, affordability, and quality outcomes.
Fragmentation across financing and delivery structures can produce uneven access and duplicated services. Integrated structures reduce these risks through unified networks and shared data.
Classification
- Financing models: Beveridge, Bismarck, National Health Insurance, Out-of-Pocket.
- Payment-model structure domain: Core models (fee-for-service, capitation, bundled/episode-based), supplementary models (pay-for-performance, shared savings, retainer-based), and organizational models (ACO, medical home) used in mixed combinations.
- Economics lens: Macroeconomics evaluates society-level spending decisions; microeconomics evaluates organizational and individual financial decisions.
- Hybrid-model implementation: National systems may follow one dominant model, while U.S. delivery mixes model elements by payer and setting.
- Cost-driver lens: Intrinsic drivers (aging demographics, chronic-disease burden, demand growth) and extrinsic drivers (technology, prescription pricing, workforce costs, policy environment).
- Pharmaceutical supply-chain domain: Medication availability depends on global raw-material sourcing, manufacturing capacity, distributor logistics, and regulatory oversight continuity.
- PBM pricing-intermediary domain: Pharmacy benefit managers negotiate drug prices and formulary access between manufacturers, insurers/employers, pharmacies, and government programs.
- Drug-price escalation drivers: Limited competition/monopoly conditions, high development costs and long approval timelines, severe-disease demand inelasticity, and policy influence from industry lobbying.
- Inflation-rebate policy domain: Medicare-focused inflation rebate requirements are a policy tool intended to limit excessive year-over-year price growth.
- ACA policy domain: Marketplace plan pathways, preexisting-condition protections, reduced exclusion-limit risk, preventive-service coverage rules, essential-benefit access, and insurer-appeal safeguards.
- U.S. funding-stream domain: Government funding (Medicare/Medicaid and other public programs), private insurance, and self-pay.
- Medicare structure domain: Part A (inpatient/skilled nursing/hospice/some home health), Part B (outpatient/provider/preventive services), Part C (private Medicare Advantage combining A/B and often D), and Part D (prescription coverage with plan formulary variation).
- Medicaid structure domain: Joint federal-state low-income coverage with state-level service variation and ACA-linked expansion pathways.
- Other public-coverage domain: CHIP, military/veteran systems, and other federally/state-supported special-population programs.
- Insurance-plan design domain: HMO, PPO, POS, and HDHP/HSA structures with different tradeoffs in premium, network flexibility, referral/preauthorization burden, and upfront cost sharing.
- Cost-sharing domain: Deductible and copay requirements influence whether insured clients can practically use needed care.
- Ownership structures: For-profit, not-for-profit, state/local government.
- Institution types: Public institutions, private institutions, and federally run service systems.
- Delivery design: Stand-alone sites versus integrated delivery systems (IDS).
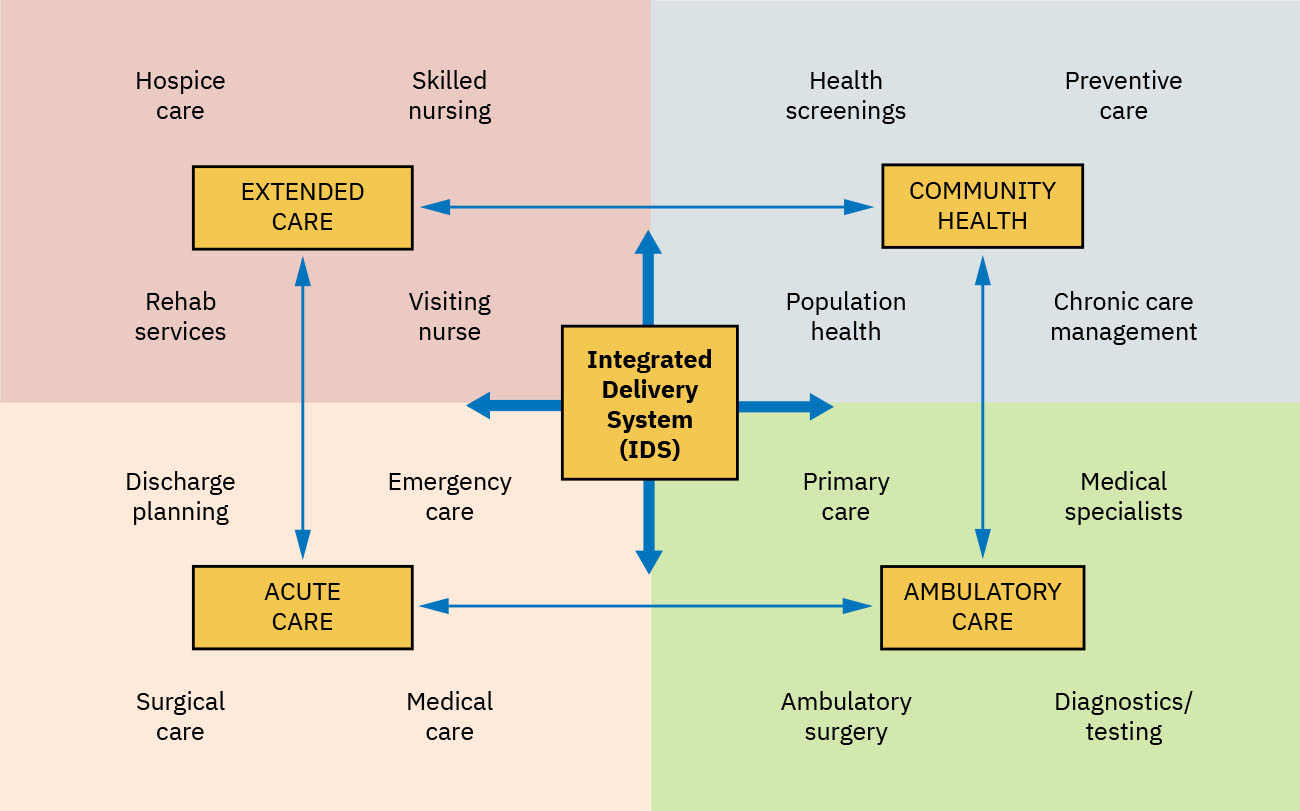 Illustration reference: OpenStax Fundamentals of Nursing Ch.3.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.3.2.
- Service-continuum domain: Inpatient acute care, subacute skilled services, outpatient/ambulatory care, post-acute recovery support, and community adult-care services.
- Care-desert domain: Regions with limited hospitals/clinics, specialist access, trauma access, maternal services, or pharmacy services; often worsened by rural hospital closure and workforce shortage.
- Community-support service domain: Home health, hospice, infusion therapy, adult day care, and in-home assistance have distinct skill scope and supervision requirements.
- Public-agency support domain: Medicare/Medicaid-linked programs and state-local agencies (for example aging and disability services) help bridge access gaps with state-level variation.
- Organizational decision test: Funding source, profit expectation/disposition, tax status, and safety-net obligation define operational type.
- Care-level governance pattern: Some systems keep primary/secondary/tertiary roles in separate practitioner tracks, while others allow fluid cross-level practice.
- For-profit profile: Investor-funded, tax-paying institutions with shareholder return expectations and lower routine safety-net scope.
- Not-for-profit profile: Tax-exempt institutions with community-service and charity-care expectations; profits are reinvested rather than distributed.
- State/local government profile: Publicly funded, tax-exempt institutions with explicit safety-net responsibilities for uninsured or underinsured populations.
- Public-versus-private operational lens: Public institutions are government-run and population-oriented; private institutions are non-government run and include both for-profit and not-for-profit entities.
- Public-health governance layer: Federal and state/local public-health agencies set policy and oversight conditions affecting all delivery organizations.
- Policy-versus-law domain: Laws are enacted regulatory rules with enforcement consequences; policies are deliberative action plans that operationalize goals across systems and organizations.
- Policy-type taxonomy domain: Public policy (government regulation), health policy (health-goal pathway), social policy (population welfare), nursing policy (practice boundaries/requirements), and institutional policy (organization-specific rules).
- Policy cultural-fit domain: Policy design should account for culture/religion/ethnicity and use trusted community leaders during planning to improve adoption and reduce inequitable impact.
- Public-health delivery-mechanism domain: Policy execution can use fiscal tools (subsidies/taxes/free services), regulation, health education/health-literacy support, preventive treatment pathways, and screening programs.
- State/local public-health operations: Immunization and family services, communicable-disease surveillance/reporting, emergency preparedness, and community vital-record workflows.
- IDS function profile: Networks that share information, responsibility, and resources to coordinate primary, secondary, and tertiary care.
- Primary-care medical-home link: A practical IDS example where primary care anchors multi-level coordination.
- Nonfederal IDS profile: Community-facing systems combining hospitals and outpatient sites with shared EHR-based continuity across care levels.
- Community-hospital profile: Nonfederal hospitals serving the general public; may be integrated within larger systems or operate as stand-alone sites.
- Federal-system profile: Population-specific IDS structures (for example veteran, tribal/indigenous, and military-family systems) with eligibility-based access.
- Federal IDS examples: Veteran, tribal/indigenous, and military health systems that deliver multi-level care within dedicated networks.
- Provider-practice structure: Independent (solo) practices versus group practices, with ongoing consolidation toward larger groups in many markets.
Nursing Assessment
NCLEX Focus
Link patient barriers and care delays to system-level factors such as insurance, network structure, and referral pathways.
- Assess insurance/coverage context and likely affordability barriers.
- Assess which system type the patient is navigating (public, private, IDS, federal).
- Assess referral pathway complexity and risk of service fragmentation.
- Assess continuity threats during cross-organization transitions.
- Assess equity implications for underserved populations.
- Assess whether patients are confusing levels of prevention with levels of care, which can distort expectations and care navigation.
- Assess likely transfer destination if the current institution is not functioning as a safety-net site.
- Assess risk that profit-driven service lines or site closures may reduce local access, especially in rural settings.
- Assess whether uninsured/underinsured patients may face stabilization-then-transfer workflows and prepare continuity safeguards.
- Assess federal-system eligibility (for example veteran, tribal affiliation/service pathways, military family status) before assuming standard community-network referral options.
- Assess whether local provider market is dominated by large groups versus independent practices, because availability and after-hours access patterns may differ.
- Assess whether local care plans are increasing cost burden without clear outcome gain and escalate value-review concerns through quality channels.
- Assess whether insured patients still face practical affordability barriers (premium burden, deductibles, noncovered drugs, or formulary restrictions).
- Assess whether a patient’s plan structure (for example HMO referral limits or high deductible) is blocking timely diagnostics, specialist access, or medication pickup.
- Assess Medicare/Medicaid eligibility context and state-variation effects before assuming uniform benefits.
- Assess whether the patient’s current needs are best matched to inpatient, subacute, outpatient, post-acute, or community-based adult-care services.
- Assess whether patients and caregivers understand the difference between skilled home health services and non-skilled in-home assistance.
Nursing Interventions
- Guide patients through system navigation and referral processes.
- Coordinate with case management for network, coverage, and access barriers.
- Use integrated records and structured handoff to reduce duplication.
- Escalate system barriers affecting timely care delivery.
- Support patient-centered planning that fits real coverage and resource constraints.
- Teach that prevention levels (primary/secondary/tertiary prevention) are action domains and are not synonymous with care-level complexity.
- Pre-brief patients on probable stabilization-and-transfer pathways when institutional safety-net scope is limited.
- Activate state/local public-health resources when preventive services or safety-net access is needed beyond hospital-based care.
- Verify charity-care and coverage-support pathways early when organization type predicts financial barriers.
- Use shared-record capability in integrated systems to reduce duplicate diagnostics and transition information loss.
- For federal-system-eligible patients, route referrals within the same IDS when feasible to preserve benefit alignment and continuity.
- Route eligible patients to state/local public-health programs (for example vaccination, family services, or reportable-condition follow-up) to close prevention and continuity gaps.
- In cost-sensitive planning, prioritize interventions and technologies with stronger outcome benefit relative to added cost and avoid low-value duplication.
- For ACA/Marketplace-covered patients, verify plan-network and formulary fit early and assist with insurer-appeal pathways when indicated.
- For self-pay or underinsured patients, refer early to case management/social work/financial counselors for Marketplace or public-program screening.
- During discharge planning, align recommended follow-up sites and medications with the patient’s actual network and cost-sharing constraints.
- Connect eligible patients and caregivers to community and public-agency supports (for example aging services, waiver pathways, and local adult-care resources) to sustain home and post-acute care plans.
- Match target outcomes to the most suitable delivery mechanism (fiscal, regulatory, education, preventive treatment, or screening) and define measurement before rollout.
- When designing or implementing policy in diverse communities, engage cultural-group leaders early to validate values, acceptability, and practical implementation barriers.
- For medication-access planning, include drug-supply reliability checks and early contingency pathways (formulary alternatives, therapeutic substitutions, and refill continuity planning) when shortages or price spikes threaten treatment adherence.
System-Blind Planning
A clinically correct plan can still fail if delivery-model constraints and access barriers are not addressed.
Pharmacology
Medication access is strongly affected by coverage model and formulary structure; nurses should anticipate affordability and access barriers when planning treatment.
Clinical Judgment Application
Clinical Scenario
A patient receives specialty recommendations but misses follow-up due to network confusion and cost concerns.
- Recognize Cues: Care plan failure is linked to system navigation and affordability barriers.
- Analyze Cues: Structural factors, not only patient motivation, are driving nonadherence.
- Prioritize Hypotheses: Priority is redesigning plan to match delivery-model realities.
- Generate Solutions: Engage care coordination, verify network options, and simplify referral path.
- Take Action: Implement revised system-aligned follow-up plan.
- Evaluate Outcomes: Attendance and continuity improve.
Related Concepts
- levels-of-care-primary-secondary-and-tertiary-framework - Operational movement through system tiers.
- patient-care-coordination-interdisciplinary-referrals-and-case-management - Team workflow for structural complexity.
- communication-barriers-emotional-intelligence-and-bias-awareness - Communication factors that amplify system barriers.
Self-Check
- How do financing models influence patient access to care?
- Why do integrated delivery systems often improve continuity?
- Which nursing actions best reduce harm from organizational fragmentation?