Communication Barriers Emotional Intelligence and Bias Awareness
Key Points
- Communication barriers can be physical, emotional, perceptual, cultural, or interpersonal.
- Emotional intelligence (EI) strengthens self-regulation, empathy, and relationship management.
- Implicit bias and stereotyping can silently degrade assessment and communication quality.
- Barrier-aware teaching improves comprehension, follow-through, and patient safety.
- Hierarchical power imbalance and retaliation fear can suppress speaking up and delay safety escalation.
- Generalizations may inform initial questions, but stereotype-driven assumptions about individuals undermine culturally safe communication.
Pathophysiology
Communication barriers are human-factors risks in healthcare systems. They interrupt message transfer, distort interpretation, and delay safe action.
EI provides protective regulation mechanisms by improving self-awareness, self-management, and social-response quality during high-stress interactions.
Classification
- Physical barriers: Noise, distance, time constraints, sensory/language mismatch.
- Physical-subtype barriers: Environment disruption, stimuli/noise, space configuration/privacy limits, time delays, distance/access limits, technical failures, and information-overload volume.
- Physiological barriers: Pain, fatigue, and sedative effects that impair message reception and recall.
- Emotional barriers: Anxiety, anger, fear, pride, overwhelm.
- Perceptual barriers: Expectations, triggers, personal experiences, assumptions.
- Cultural-conflict trigger domain: Mismatch in values, beliefs, communication styles, and care expectations can escalate conflict and reduce trust.
- Interaction-style barriers: Disengaged/condescending tone, excessive probing, and interrogative “why” framing that trigger defensiveness.
- Bias barriers: Implicit bias, stereotyping, and prejudgment.
- Generalization-versus-stereotype barrier: Group-level patterns can be starting points for inquiry, but fixed assumptions about an individual can distort assessment and rapport.
- Bias expression spectrum: Explicit bias (consciously held) and implicit bias (automatic/unconscious) can both impair care.
- Bias-mitigation methods domain: Stereotype replacement, counter-stereotypic imaging, evaluative conditioning, individuation, perspective taking, identifying self with the outgroup, and cultural immersion/engagement can reduce bias expression.
- Cultural/interpersonal barriers: Cultural mismatch, low humility, weak relationship management.
- Organizational power barriers: Hierarchy-driven communication limits and fear of retaliation that inhibit safety reporting.
- Nurse-client power-imbalance domain: Differences in role authority and clinical knowledge can suppress client voice, especially when communication style becomes authoritarian.
- Interprofessional-collaboration barriers: Differences in professional language/jargon, schedules/routines, preparation and status, education/regulatory norms, accountability/reimbursement models, role complexity, rapid decision pressure, and profession-identity rivalry.
- Auditory-communication barriers: Hearing-aid malfunction, poor lighting for lip-reading/visual cues, mask-related lip-reading limits, and ASL-English interpretation mismatch.
- EI domains: Self-management, self-awareness, social awareness, and relationship management.
- EI-versus-CQ domain: EI focuses on emotional awareness and regulation in self/others, while CQ focuses on culturally adaptive knowledge, skills, and behavior across cultural contexts.
- CQ component domain: Cultural knowledge, cultural understanding, cultural skills, and cultural adaptability.
- Blind-spot domain: Unrecognized implicit assumptions can influence judgment and behavior without conscious intent.
- Mindful-awareness domain: Nonjudgmental present-moment attention supports cultural humility, empathic listening, and conflict de-escalation.
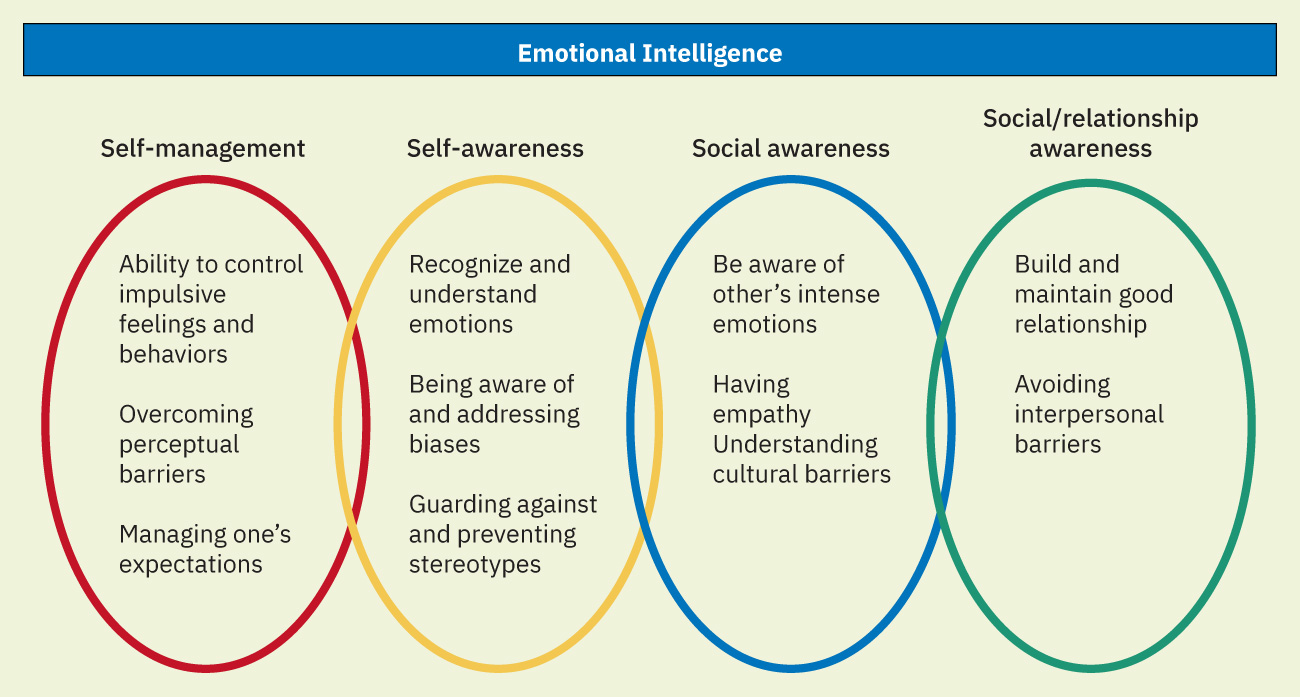 Illustration reference: OpenStax Fundamentals of Nursing Ch.2.5.
Illustration reference: OpenStax Fundamentals of Nursing Ch.2.5.
Nursing Assessment
NCLEX Focus
Identify the primary barrier type first, then choose the communication adaptation with the highest immediate safety benefit.
- Assess environment for noise, privacy gaps, and language-access needs.
- Assess physical-setting barriers including thin-wall privacy risk, delayed return-to-patient timing, distance/access limits, and device/connectivity problems.
- Assess emotional state and signs of communication shutdown.
- Assess both patient-side and provider-side emotional barriers (fear, pride, anger, anxiety) that may distort message exchange.
- Assess for sensory-access barriers and verify use of needed hearing or vision assistive devices.
- Assess hearing/vision-specific communication needs (for example captioned video, TTY, large-print, audio, screen-reader, or Braille-compatible formats).
- Assess hearing-specific readiness before critical teaching (for example hearing aid availability/function, room lighting, distraction control, and whether qualified sign-language interpretation is needed).
- Assess for expectation mismatch and unresolved fear-based assumptions.
- Assess expectation gaps early (for example recovery timeline or symptom trajectory) to reduce preventable emotional escalation.
- Assess personal and team bias risks that may affect tone or decision quality.
- Assess conflict risks caused by value, belief, and communication-style mismatch before high-stakes discussions.
- Assess whether team hierarchy is limiting open communication or suppressing safety concern escalation.
- Assess for nurse-client power imbalance cues such as deference, fear of questioning, or reduced disclosure when authority pressure is perceived.
- Assess whether staff report fear of embarrassment, retaliation, or social penalty when speaking up.
- Assess whether team communication is fragmented by schedule mismatch, role-status gradients, or accountability-model differences.
- Assess whether questioning style is causing client defensiveness (for example repeated “why” questions or rapid-fire probing).
- Assess for automatic judgment, emotional reactivity, or attention drift that may reduce culturally respectful communication.
- Perform a pre-encounter self-check for stigma-trigger topics (for example substance use, mental illness, teen pregnancy, STI status, or sexual/gender minority identity).
- Assess patient learning using preferred communication mode and teach-back.
- Assess for information overload and stop-point cues before adding new education content.
Nursing Interventions
- Remove or reduce physical barriers before critical teaching or consent discussions.
- Use backup communication pathways (written reinforcement, quieter venue, or technical support) when noise or equipment barriers disrupt understanding.
- Use trained medical interpreters for language discordance.
- Do not use family members as default interpreters for clinical decision-making, especially for sensitive or high-risk discussions.
- Choose interpreter modality based on encounter needs: in-person for complex/high-emotion encounters when feasible, phone for rapid access, and video when visual cues improve comprehension.
- For interpreter-mediated encounters, pre-brief when feasible, allow extra time, speak directly to the patient in first person, avoid idioms/slang, and document interpreter identity in the progress note.
- When discussing sensitive topics, consider matching interpreter gender preference when possible to reduce embarrassment barriers.
- For culturally sensitive subjects, normalize the topic briefly and ask permission before proceeding.
- Apply EI practices: pause, self-check, empathetic response, and adaptive tone.
- Practice staff self-management and recovery routines after emotionally intense encounters to preserve communication quality.
- Use periodic self-audit tools (for example reflection journaling or validated implicit-bias screens) to surface hidden assumptions.
- Use targeted bias-interruption techniques (for example stereotype replacement, counter-stereotypic imaging, individuation, and perspective taking) during care planning and communication.
- Seek regular cross-cultural contact and reflection opportunities to reduce outgroup assumptions and strengthen culturally adaptive communication.
- Use a brief centering pause (for example, one deep breath) before entering busy encounters to restore full attention.
- Use mindful listening by intentionally focusing on the speaker, delaying judgment, and reflecting the patient’s perspective before offering recommendations.
- Set one clear goal for high-stakes conversations and adjust communication pace/tone when cues show emotional overload.
- Optimize interview setup with eye-level positioning, direct eye contact, and unhurried presence to improve cue recognition.
- Control ambient conditions (noise and lighting) and prefer face-to-face delivery for high-stakes messages to preserve nonverbal context.
- Use telehealth or remote specialist communication strategically when distance barriers limit timely in-person access.
- Adapt scheduling and pacing to the patient’s time-orientation and practical access constraints when feasible.
- Reduce preprocedure communication overload by consolidating contacts, prioritizing action steps, and co-creating simple call/task sequences.
- For hearing barriers, reduce competing background noise and use captioned or text-supported communication options.
- For hearing impairment communication, face the patient in good light, speak clearly without shouting, and use intentional gesture/visual support while maintaining natural articulation.
- Use qualified sign-language interpreters when needed and avoid relying on ad hoc family translation for deaf or hard-of-hearing clinical communication.
- Do not rely on writing alone for complex or urgent communication, especially when literacy or emergency pace may limit understanding.
- For visual barriers, optimize lighting and provide audio/large-print/magnification support as needed.
- For severe language barriers, yes/no prompts can be used briefly for urgent basic information while arranging full interpreter-supported assessment.
- Treat reversible physiologic barriers (for example pain) before teaching; avoid obtaining legally significant signatures after sedating medication.
- When stress signs appear (irritability, palpitations, poor concentration), use simple relaxation breathing or progressive muscle relaxation before continuing.
- Address bias through deliberate reflection and standardized communication routines.
- Use structured speak-up and escalation scripts so staff can raise high-risk concerns consistently across hierarchy levels.
- Coach leaders to acknowledge concerns without dismissal and to reinforce psychological safety after escalations.
- Use shared decision-making language and option framing so clients can participate in choices aligned with their values and preferences.
- Reinforce client rights and autonomy by inviting questions, confirming understanding, and explicitly validating the client’s role in final care decisions.
- Train mixed-discipline teams together on structured communication tools and plain-language expectations to reduce role-identity silos.
- Name and challenge explicit discriminatory language or behavior immediately using policy-supported escalation pathways.
- Individualize teaching format (visual, verbal, written, demonstration) to patient needs.
- Match patient-teaching materials to communication accommodations (for example large print, audio, Braille, or accessible electronic formats) and verify learning with restatement or return demonstration.
- Document barriers identified, strategies used, patient response, and remaining learning needs for continuity across team members.
Unchecked Bias Hazard
Implicit bias can produce subtle communication inequities that delay diagnosis, reduce trust, and worsen outcomes.
Pharmacology
Medication education should account for emotional load and bias risk; misunderstanding of dosage, timing, and side effects is more likely when barriers are unaddressed.
Clinical Judgment Application
Clinical Scenario
A preoperative patient appears disengaged, misses preparation calls, and gives brief answers during assessment.
- Recognize Cues: Communication avoidance and possible emotional overload.
- Analyze Cues: Emotional and logistical barriers are likely limiting engagement.
- Prioritize Hypotheses: Priority is restoring psychological safety and practical navigation support.
- Generate Solutions: Use reflective listening, simplify next steps, and co-create a call/appointment plan.
- Take Action: Coordinate support resources and confirm understanding via teach-back.
- Evaluate Outcomes: Patient engagement improves and preparation milestones are completed.
Related Concepts
- health-literacy-assessment-and-plain-language-education - Barrier-adapted teaching and verification.
- culturally-competent-care - Cultural alignment and humility in communication.
- therapeutic-communication-and-relationships - Relational techniques that reduce emotional barriers.
Self-Check
- Which barrier type should be addressed first when immediate safety communication is needed?
- How does emotional intelligence reduce communication breakdown under stress?
- What practical strategies reduce the impact of implicit bias in nursing communication?