Levels of Care Primary Secondary and Tertiary Framework
Key Points
- Primary care emphasizes prevention, early identification, and routine management.
- Secondary care addresses focused acute or specialty needs and stabilizes patient status.
- Tertiary care delivers advanced diagnostics, invasive procedures, and major-surgery management for severe or highly complex conditions.
- Safe care requires planned movement between levels with clear referral and return-to-primary pathways.
- Patients may enter at secondary care when access barriers delay primary evaluation, increasing risk and cost.
- Primary, secondary, and tertiary prevention are action levels that can occur across multiple care settings, not fixed facility tiers.
- Tertiary prevention for chronic illness should preserve function and quality of life through rehabilitation, symptom control, and continuity follow-up.
Pathophysiology
Levels of care represent a healthcare delivery design, not a biologic disease process. Patients move between levels based on complexity, acuity, and required expertise.
Care failures commonly occur at transition points when referral intent, treatment goals, and follow-up responsibilities are not clearly communicated.
Classification
- Primary care: Health promotion, prevention, screening, and routine chronic care.
- Primary care first-contact role: Usual entry point for new concerns, annual exams, immunizations, and common mild-to-moderate problems.
- Primary care continuity role: Ongoing relationship over time that supports early detection, reduced downstream cost, and safer escalation when complexity increases.
- Primary care medical-home role: Comprehensive coordination hub that connects specialty referrals and preserves quality/safety across levels.
- Primary care service breadth: Broad outpatient procedures/services (for example basic lab testing, injections, x-rays, minor wound care, nutrition counseling, and chronic-condition follow-up).
- Primary care setting diversity: Offices, walk-in/urgent sites, pharmacies, school-based services, and community outreach settings.
- Secondary care: Specialist evaluation and management of more complex acute/chronic problems with a goal of stabilization, education, and return to baseline.
- Secondary care access pattern: Usually referral-based but also direct unscheduled entry through emergency/urgent presentation.
- Secondary care clinical profile: Organ-focused, generally noninvasive or minimally invasive services (for example advanced imaging, specialty testing, same-day procedures, focused therapies, and crisis mental-health care).
- Tertiary care: Highest-complexity care for severe, rare, or multi-comorbidity conditions requiring highly specialized staff, advanced technology, and invasive or major procedural care.
- Secondary-tertiary provider overlap: Disciplines may overlap, but tertiary providers add advanced management scope (for example operative or critical-care specialization).
- Tertiary care availability pattern: Fewer facilities than secondary care, often concentrated in large urban or specialty centers with transport from other sites when needed.
- Tertiary care treatment arc: Usually specific and time-bounded around severe events; care is handed back to secondary/primary teams after stabilization or definitive treatment.
- Tertiary setting spectrum: Level 1 trauma and specialty hospitals are common, but tertiary intensity can also occur in specialized outpatient programs when team expertise and intensity are high.
- Transition pattern: Escalation for complexity, then de-escalation back to continuity care.
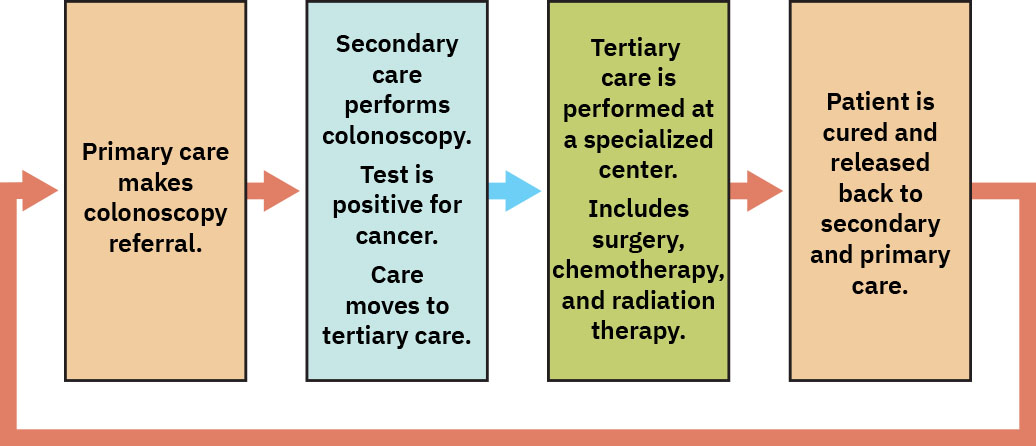 Illustration reference: OpenStax Fundamentals of Nursing Ch.3.1.
Illustration reference: OpenStax Fundamentals of Nursing Ch.3.1.
- Prevention-versus-care distinction: Primary/secondary/tertiary prevention are action levels and are not equivalent to primary/secondary/tertiary care settings; tertiary prevention may be provided in primary care.
- Primary-prevention action domain: Disease-before-onset prevention through immunization, healthy-lifestyle support, and injury-risk reduction.
- Secondary-prevention action domain: Early detection and early treatment through screening and timely intervention.
- Tertiary-prevention action domain: Ongoing disease-impact reduction through chronic-care management, rehabilitation services, symptom-control treatment, and scheduled follow-up after diagnosis.
Nursing Assessment
NCLEX Focus
Prioritize where the patient should receive care now and what transition details are required for safety.
- Assess current acuity, stability, and urgency to determine care-level fit.
- Assess whether current setting can provide required diagnostics/interventions.
- Assess referral indications and urgency for specialist or tertiary services.
- Assess discharge/readiness factors for return to lower level with follow-up.
- Assess patient understanding of why transitions are occurring.
- Assess whether the patient has reliable primary-care attachment; absent PCP linkage increases late, higher-acuity entry risk.
- Assess access barriers (transportation, appointment availability, insurance/coverage, rural availability, fear/delay) that may shift entry from primary to secondary care.
- Assess whether the needed intervention exceeds secondary capability (for example major surgery, advanced subspecialty diagnostics, or intensive multi-comorbidity management) and therefore requires tertiary transfer.
- Assess medication-fragmentation risk when multiple specialists are active, especially in older adults with multimorbidity.
Nursing Interventions
- Coordinate timely referrals with complete clinical context and rationale.
- Clarify goals of each level and expected handoff outcomes.
- Educate patient/family about where to seek routine vs urgent vs specialized care.
- Clarify that prevention action level and care delivery level can differ in the same encounter.
- Teach concrete prevention examples by level (primary: immunization/lifestyle risk reduction; secondary: screening and early treatment; tertiary: rehab/chronic-condition self-management support).
- In secondary-prevention counseling, specify age and risk triggers for screening escalation, including earlier schedules when family-history or genetic risk is present.
- Confirm return pathway to primary care after specialty episodes.
- Document transition decisions and contingency instructions.
- Reinforce primary-care access points beyond physician offices (for example walk-in clinics, urgent care, pharmacies, and school-based services) when appropriate.
- Frame secondary referrals as time-limited problem-focused episodes when clinically appropriate, and specify follow-up ownership when care transitions back to the PCP.
- For tertiary escalation, initiate rapid transfer logistics, communicate severity risk clearly, and provide family updates during transport planning.
- Predefine post-tertiary handback plans (secondary specialty follow-up plus primary continuity) before discharge from high-complexity centers.
- When chronic disease is diagnosed, coordinate tertiary-prevention services early (for example PT, OT, medication/symptom follow-up, and function-preservation planning) before discharge.
- Use a PCP-led medical-home model for patients with multiple chronic conditions to centralize medication review and reduce cross-specialty treatment conflicts.
Transition Fragmentation
Escalating care without a clear return and follow-up plan increases readmission and missed-care risk.
Pharmacology
Medication regimens often change during secondary/tertiary episodes; reconciliation and clear post-transition instructions are essential before return to primary care.
Clinical Judgment Application
Clinical Scenario
A patient seen in primary care for worsening dyspnea requires urgent specialist intervention and possible procedural management.
- Recognize Cues: Symptoms exceed routine management threshold.
- Analyze Cues: Secondary or tertiary resources are needed for definitive workup/treatment.
- Prioritize Hypotheses: Immediate safe escalation is priority.
- Generate Solutions: Arrange urgent referral and communicate risk details to receiving team.
- Take Action: Transfer with complete handoff and stabilization steps.
- Evaluate Outcomes: Specialized care is delivered, then follow-up is reconnected to primary care.
Related Concepts
- patient-care-coordination-interdisciplinary-referrals-and-case-management - Operational pathway for transitions.
- continuity-of-care-during-evaluation-phase - Ensures stable follow-through after level changes.
- nurse-licensure-compact-and-multistate-practice - Relevant when care transitions cross jurisdictions.
Self-Check
- What clinical factors most strongly determine escalation from primary to secondary care?
- Why must tertiary episodes include explicit return-to-primary planning?
- Which handoff elements prevent avoidable transition-related harm?