Effective Professional Communication and Motivational Interviewing
Key Points
- Effective nursing communication is factual, practical, clear, concise, and appropriately persuasive.
- Professional communication includes understanding, respectful title/pronoun use, trustworthiness, assertiveness, and resolution.
- Nonverbal delivery (tone, pace, body language, eye-level presence) often shapes message impact more than words alone.
- Motivational interviewing (MI) supports behavior change without coercion.
- OARS skills (open questions, affirmations, reflective listening, summaries) improve shared decision-making.
- MI is especially useful in contemplation-stage ambivalence, where “yes, but…” statements often reveal the key barrier to change.
- Organized interprofessional communication improves collaborative planning and reduces coordination gaps.
- Professional communication quality is strengthened by courtesy, empathy, and transparent resolution behaviors during routine care and adverse-event discussions.
- Interprofessional communication reliability depends on plain-language exchange, respectful confidence, active listening, and timely constructive feedback across role and hierarchy differences.
- RN communication standards include language-access support, disability-adapted communication strategies, and explicit message-understanding verification.
- Team communication becomes more reliable when role responsibilities are explicit and teams use regular check-ins to identify coordination gaps early.
Pathophysiology
Communication effectiveness is a care-quality determinant rather than a biologic process. Poorly structured messages reduce trust and adherence, while clear and patient-aligned communication improves decision quality and outcomes.
MI reduces resistance by shifting from directive persuasion to collaborative exploration of patient values, readiness, and barriers.
Classification
- Effective communication elements: Factual, practical, clear/concise, persuasive.
- Professional elements: Understanding, respectful naming/titles, trustworthiness, assertiveness, resolution.
- Assertive style: Fact-plus-feeling “I” messages that protect both parties’ rights without hostile blame.
- Behavior-change method: Motivational interviewing using OARS.
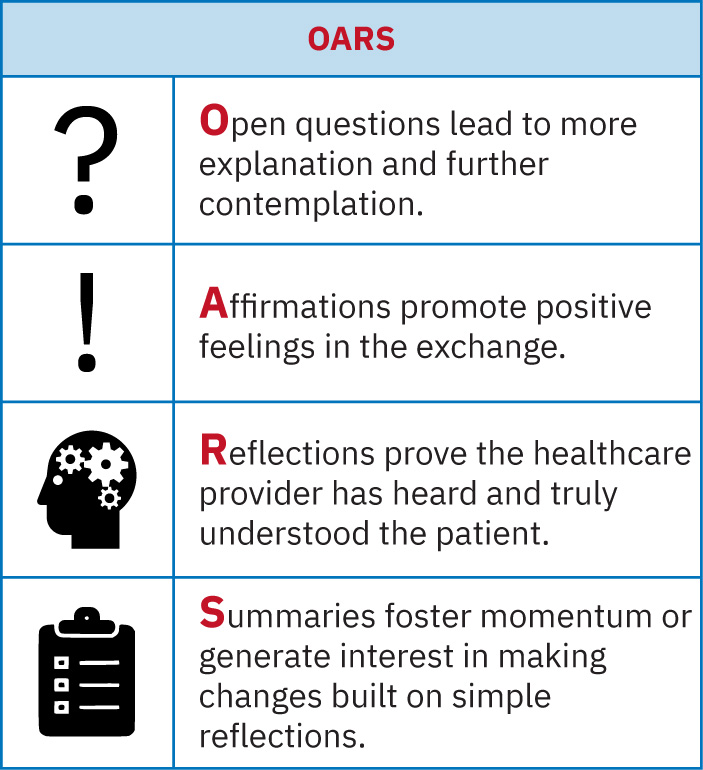 Illustration reference: OpenStax Fundamentals of Nursing Ch.2.4.
Illustration reference: OpenStax Fundamentals of Nursing Ch.2.4.
- MI principle set: Express empathy, highlight discrepancy, adjust to resistance without argument, support self-efficacy, and resist unsolicited advice reflex.
- MI process sequence: Engage, focus, evoke, and plan.
- MI stage-of-change context: Precontemplation, contemplation, preparation, action, and maintenance.
- Goal framework: SMART-style communication for actionable care planning.
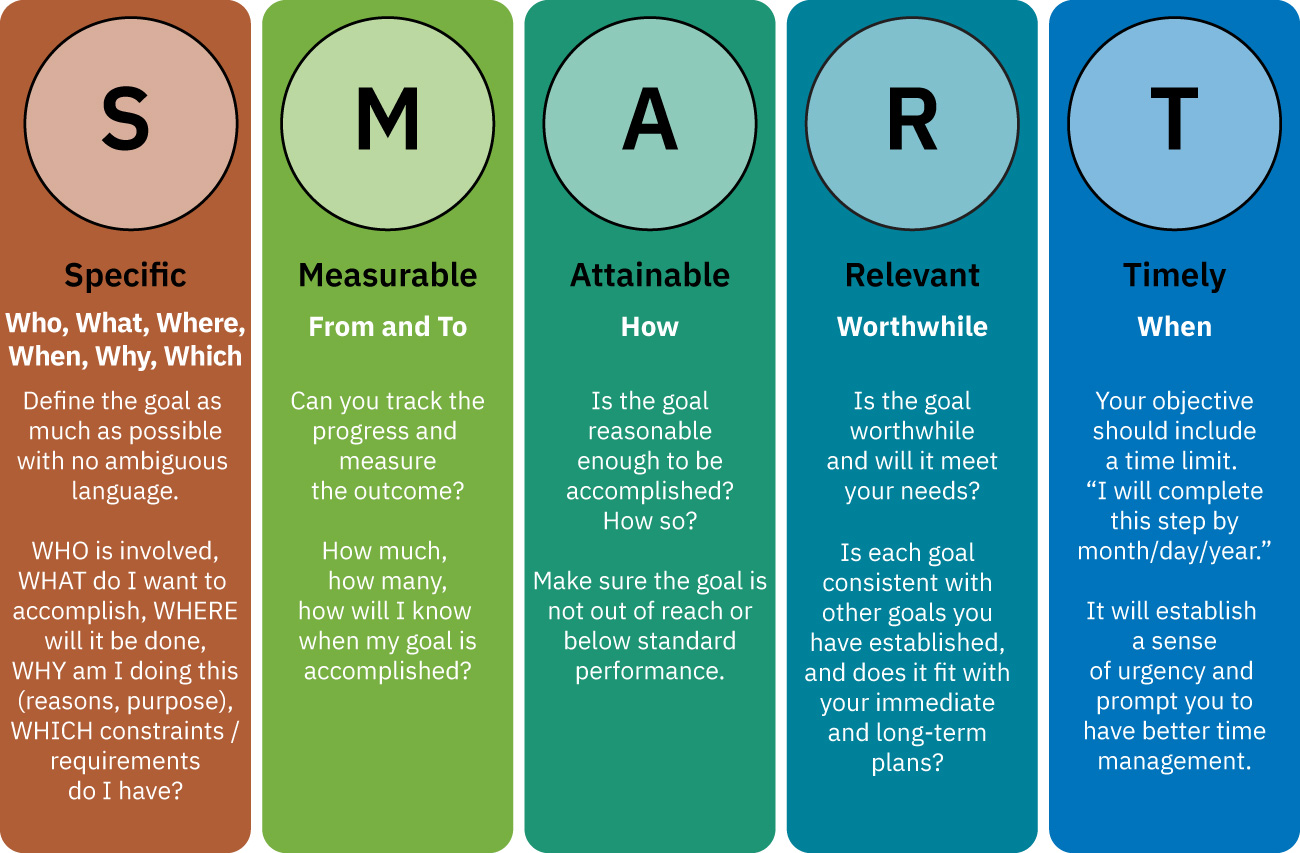 Illustration reference: OpenStax Fundamentals of Nursing Ch.2.3.
Illustration reference: OpenStax Fundamentals of Nursing Ch.2.3.
- IPEC interprofessional-communication behavior domain: Select effective communication tools (including information systems/technology), avoid discipline-specific jargon when possible, communicate with confidence/clarity/respect, listen actively, and give timely sensitive feedback.
- Role-clarity communication domain: Defining team-member role ownership and expected responsibilities reduces missed tasks and delayed follow-up.
Nursing Assessment
NCLEX Focus
Prioritize communication that clarifies patient goals and readiness before selecting education or behavior-change strategy.
- Assess whether message content is accurate and practical for patient context.
- Assess patient understanding, concerns, and priority agenda.
- Assess response quality after each interaction and identify whether communication goals were met.
- Assess surroundings, comfort, and available teaching tools before education sessions.
- Assess readiness for change and ambivalence around recommendations.
- Assess for ambivalence language (for example “yes, but…”) and identify the barrier expressed after “but.”
- Assess cultural values, general literacy, and health literacy factors that may influence motivation and change planning.
- Assess verbal and nonverbal congruence, including tone, pace, posture, and eye contact.
- Assess for verbal-nonverbal mismatch and plan follow-up questions when cues conflict.
- Assess whether privacy and distraction control are adequate before obtaining sensitive admission information.
- Assess team communication tone for trust and assertive safety advocacy.
- Assess whether conflict has reached actionable resolution.
- Assess whether the nurse needs pre-session knowledge or skill refresh before teaching high-risk procedures.
- Assess whether discipline-specific jargon is creating understanding gaps for patients, families, or non-nursing team members.
- Assess whether hierarchy, role identity, or experience-level differences are suppressing two-way communication.
- Assess need for language translation resources and for alternative communication methods when visual, speech, or language limitations are present.
- Assess whether role ownership and expected responsibilities are clearly assigned across the team for current care priorities.
Nursing Interventions
- Deliver information in short, structured, plain-language sequences.
- Convert medical terminology into lay language before introducing complex procedural or medication details.
- Build the message around receiver factors (language, sensory status, cognition, education level, and cultural preference) before delivery.
- Use OARS to explore barriers and elicit patient-owned goals.
- When ambivalence appears, explore the “yes, but…” barrier directly and co-design a plan around that obstacle.
- Use MI principles intentionally, especially in contemplation-stage clients: empathize, contrast current behavior with personal goals, and avoid argument-based persuasion.
- Use MI in sequence: engage relationally, focus the agenda, evoke patient change talk, then plan small achievable next steps.
- For initial or sensitive exchanges, position at eye level and use SOLER-aligned nonverbal presence (open posture, lean in, eye contact, relaxed manner).
- Reduce environmental distractions (noise, extra visitors, television) before focused therapeutic communication.
- Avoid cultural generalizations; ask direct, respectful questions to clarify individual practices and preferences.
- Keep verbal and nonverbal signals congruent and use active two-way feedback checks during the interaction.
- When patients fear routine procedures, explain why monitoring is ordered, what each step feels like, and how often reassessment may be needed.
- Apply assertive communication when safety concerns require escalation.
- Use “I feel…/Help me understand…” framing instead of accusatory “you” messages during conflict.
- When resistance appears (defensiveness, avoidance, interruptions), validate feelings and redirect to client-defined motivations rather than escalating advice.
- Use respectful naming and pronoun preferences to strengthen therapeutic alliance.
- When team members use incorrect pronouns or binary assumptions, provide brief corrective feedback and restate patient-identified terms in real time.
- Start encounters with a courteous greeting and maintain empathy-forward language while clarifying goals and concerns.
- Summarize agreements and document clear next steps.
- Share relevant assessments, treatment-plan changes, and progress updates with team members using concise closed-loop communication.
- Select communication channel/tool based on urgency and team function needs (for example direct verbal escalation plus EHR documentation for high-risk changes).
- Use plain-language explanations in interprofessional discussions when technical jargon could obscure shared understanding.
- Deliver timely, respectful, and behavior-specific feedback to support team performance and communication recovery.
- Use regular interdisciplinary check-ins to confirm role execution, identify emerging problems, and correct workflow drift before patient harm occurs.
- Confirm key messages were heard and understood by the intended recipient before closing safety-critical communication.
- Disclose and report potential or actual care hazards/deviations from standard care through established safety channels.
- End with an explicit invitation for additional concerns so patients can request unresolved help.
- Offer pacing control (for example, “we can go slowly”) and supportive options (family call/visit) to reduce anxiety and preserve cooperation.
- Use accessible formats when needed (for example captioning, large print, language-matched materials, and multimodal delivery) and verify with teach-back/demonstration.
- Document clinically meaningful nonverbal cues and the intervention taken when those cues indicate unresolved concerns.
- During adverse-event communication, use direct factual disclosure, immediate safety actions, and prevention-focused follow-up planning to support resolution.
Coercive Communication Risk
Pressuring behavior change without MI principles can increase resistance and reduce adherence.
Pharmacology
Medication counseling is more effective when MI techniques are used to uncover adherence barriers and align plans with patient priorities.
Clinical Judgment Application
Clinical Scenario
A patient with chronic pain declines physical therapy and repeatedly requests medication-only treatment.
- Recognize Cues: Ambivalence, fear of worsening pain, and narrow treatment preference.
- Analyze Cues: Direct persuasion alone is unlikely to change behavior.
- Prioritize Hypotheses: MI-based engagement is needed before care-plan commitment.
- Generate Solutions: Use OARS to identify goals, concerns, and acceptable first steps.
- Take Action: Co-create a phased plan with measurable goals and follow-up.
- Evaluate Outcomes: Patient participation and plan adherence improve.
Related Concepts
- therapeutic-communication-and-relationships - Foundation for relational communication and trust.
- health-literacy-assessment-and-plain-language-education - Supports clarity and understanding.
- conflict-resolution-skills-in-nursing-management - Professional resolution in high-stakes communication.
Self-Check
- Why is “practical” communication distinct from “factual” communication?
- How does OARS reduce resistance compared with directive counseling?
- When should assertive communication be prioritized in nursing practice?