Conflict Resolution Skills in Nursing Management
Key Points
- Conflict is expected in high-stress clinical environments and must be managed, not ignored.
- Effective resolution starts with root-cause identification and structured communication.
- Nurse managers mediate toward solutions aligned with patient safety and team capability.
- Open, assertive, and respectful communication are complementary techniques that reduce escalation risk.
- Win-win outcomes are preferred but not always achievable, so safe compromise pathways are still required.
- Skillful conflict handling strengthens collaboration, trust, and care reliability.
- TeamSTEPPS conflict tools (DESC, CUS, and two-challenge) standardize safety-focused escalation across hierarchy levels.
- Style selection should match clinical context by balancing commitment to goals and commitment to relationships.
Pathophysiology
Unresolved interpersonal conflict can degrade communication quality, delay decisions, and increase near-miss risk. In contrast, constructive mediation restores psychological safety and supports coordinated care execution.
Conflict resolution in nursing management is therefore a safety and culture function, not only a relational function.
Classification
- Task conflict: Disagreement about care priorities, workflow, or treatment sequencing.
- Relationship conflict: Interpersonal tension affecting communication and teamwork.
- Process conflict: Dispute over role boundaries, delegation, or protocol interpretation.
- Common interpersonal-source domain: Passive-aggressive behavior, horizontal aggression, defensiveness, peer-informer behavior, and victimization narratives.
- Conflict-type domain: Role conflict, communication conflict, goal conflict, personality conflict, and ethical/values conflict.
- Multi-party conflict context: Staff, clients, providers, and families can all be participants in workplace conflict episodes.
- Mediated resolution: Manager-guided dialogue toward mutually acceptable action plan.
- Style-axis domain: Thomas-Kilmann model balances commitment to goals with commitment to relationships.
- Approach spectrum: Avoiding, competing, accommodating, compromising, and collaborating; no single approach is universally superior.
- TeamSTEPPS conflict-escalation domain: Assertive statement sequence, two-challenge rule, CUS safety phrases, and DESC conflict-conversation structure.
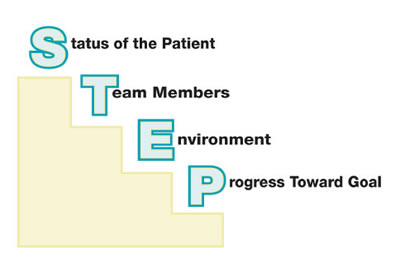 Illustration reference: OpenRN Nursing Management and Professional Concepts 2e Ch.7.6.
Illustration reference: OpenRN Nursing Management and Professional Concepts 2e Ch.7.6.
Nursing Assessment
NCLEX Focus
Priority is to protect patient safety first, then repair team function through structured mediation.
- Assess immediate patient-risk impact of the conflict.
- Assess root drivers: communication breakdown, workload imbalance, or role ambiguity.
- Assess each party’s goals, assumptions, and constraints.
- Assess whether cultural or communication-style differences are contributing to misunderstanding.
- Assess whether policy or scope-of-practice misunderstanding is involved.
- Assess if workload distribution or delegation fairness is the central trigger.
- Assess for passive-aggressive mismatch between stated agreement and observed behavior.
- Assess for horizontal aggression, bullying, or hostile peer interactions that require direct intervention.
- Assess whether conflict reports are objective and first-hand or represent peer-informer/gossip patterns.
- Assess whether perceived victimization reflects communication gaps or repeated standards nonadherence.
- Assess whether team expectations are being enforced consistently and perceived as fair across staff.
- Assess whether staff view leaders and peers as approachable for direct feedback.
- Assess predictable response style during feedback (defensiveness, deflection, or denial) to pre-plan communication.
- Assess need for follow-up coaching after initial resolution.
Nursing Interventions
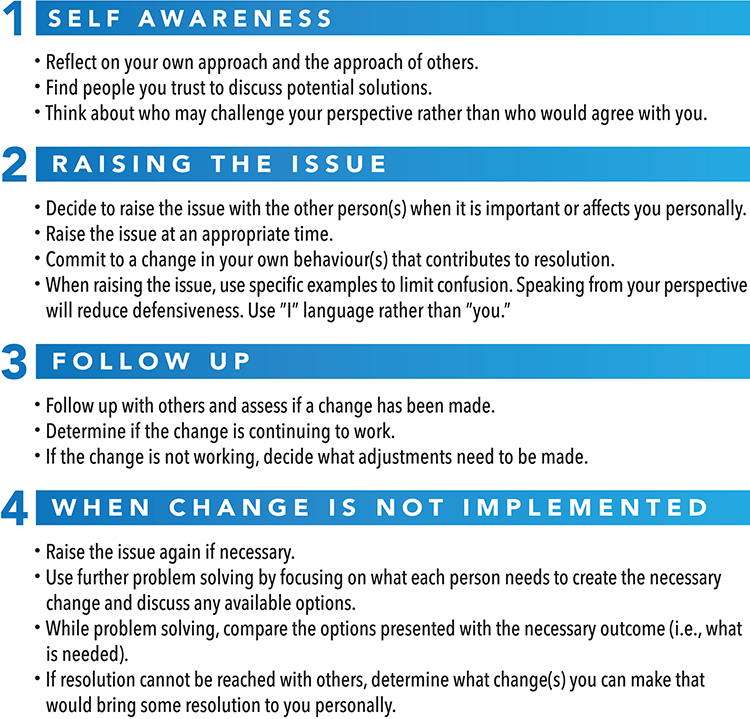 Illustration reference: OpenRN Nursing Management and Professional Concepts 2e Ch.7.7.
Illustration reference: OpenRN Nursing Management and Professional Concepts 2e Ch.7.7.
- Hold a timely, neutral discussion with clear behavioral expectations.
- Use open communication as a two-way process with explicit listening expectations.
- Coach assertive communication that is direct and honest while preserving respect for others.
- Reinforce respectful communication standards: empathy, nonverbal awareness, and concern-focused language rather than personal attacks.
- Use active listening and restatement to surface underlying concerns.
- Reframe dispute around shared patient-centered goals.
- Select conflict style by context: avoid briefly when immediate stabilization is needed, compete for urgent safety control, accommodate selectively, compromise for rapid workable middle ground, and collaborate when time/trust permit deeper resolution.
- Build integrative solutions that combine effective elements from differing care approaches when both perspectives hold value.
- Negotiate explicit agreements on responsibilities and communication steps.
- Use collaborative problem-solving first when a mutually beneficial solution is feasible.
- Use compromising when both parties can concede safely to reach a workable middle ground.
- Address passive-aggressive behavior directly and calmly by naming discrepancy between public agreement and private nonadherence.
- Redirect defensive responses to objective facts, specific safety risk, and concrete next steps.
- For peer-informer concerns without urgency, coach direct peer-to-peer conversation first; escalate when repeated reports suggest a true pattern.
- For victimization statements, reinforce consistent standards while protecting coworker confidentiality.
- Escalate up chain of command when safety risk persists or local resolution fails.
- Use avoiding only as a brief cooling-off measure; chronic avoidance weakens trust and rapport.
- Use accommodating selectively when one party is clearly in error or the counterpart has greater expertise; avoid over-accommodating against team safety interests.
- Use assertive statements for immediate safety concerns: opening, concern, problem, solution, and agreement on next steps.
- Apply the two-challenge rule when an initial safety concern is ignored; repeat concern at least twice, then escalate by chain of command if unresolved.
- Use CUS phrasing (“concerned, uncomfortable, safety issue”) during high-stress events to clearly signal an urgent safety breach.
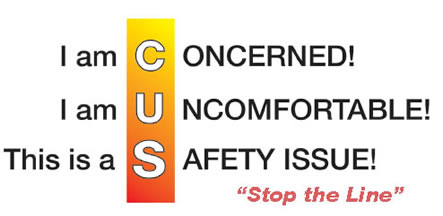 Illustration reference: OpenRN Nursing Management and Professional Concepts 2e Ch.7.6.
Illustration reference: OpenRN Nursing Management and Professional Concepts 2e Ch.7.6. - Use the DESC tool in a private area and center discussion on what is right for patient/team safety rather than who is right.
- De-escalate by reducing threat/emotional intensity, keeping focus on problem-solving, and preventing side-taking dynamics.
- Set clear team expectations in advance, reinforce them consistently, and follow up with visible accountability.
- Lead difficult conversations with the core concern first, then define performance gap, expected change, why it matters, timeline, and follow-up checkpoint.
- Anticipate defensiveness, deflection, and denial during coaching; respond with calm transparency and behavior-specific examples.
- Use team-strengths awareness and routine coaching to prevent negative attitudes from becoming entrenched conflict patterns.
- Leverage available supports (peer nurse leaders, professional development, and HR pathways) when direct mediation is insufficient.
- Document plan and revisit outcomes to prevent recurrence.
Delay Escalation Hazard
Prolonged unresolved conflict can normalize unsafe communication and increase care defects.
False Win-Win Assumption
Not all conflicts can produce a perfect win-win outcome; managers should still secure a fair, safe, and sustainable resolution.
Escalation Suppression Risk
Ignoring repeated safety concerns without chain-of-command escalation can normalize preventable harm.
Pharmacology
Conflict over medication priorities or administration timing should be mediated promptly to prevent omissions, delays, and contradictory instructions.
Clinical Judgment Application
Clinical Scenario
Two nurses disagree about whether to prioritize pain control or mobility training before discharge teaching.
- Recognize Cues: Care-priority disagreement is affecting team coordination.
- Analyze Cues: Conflict includes both task and communication components.
- Prioritize Hypotheses: Mediation can align priorities with patient goals and safety.
- Generate Solutions: Clarify evidence, sequence tasks, and define shared plan.
- Take Action: Facilitate team discussion and assign explicit follow-up roles.
- Evaluate Outcomes: Teaching and discharge workflow proceed without further conflict.
Delegation-Workload Scenario
An LPN/VN and nursing assistant dispute task distribution in long-term care, each perceiving unfair expectations.
- Recognize Cues: Conflict combines process (delegation) and relationship strain.
- Analyze Cues: Unclear workload expectations and limited acknowledgment are amplifying frustration.
- Prioritize Hypotheses: Early mediated dialogue can prevent morale decline and care inconsistency.
- Generate Solutions: Clarify role expectations, rebalance tasks, and set communication checkpoints.
- Take Action: Conduct neutral mediation with shared expectations and explicit follow-up.
- Evaluate Outcomes: Team cohesion and resident-care reliability improve.
Safety-Escalation Scenario
A nurse observes sterile technique contamination during central-line preparation and the operator dismisses the initial warning.
- Recognize Cues: Immediate procedure-related infection risk and a hierarchy barrier to speaking up.
- Analyze Cues: Single warning failed; standardized escalation language is needed.
- Prioritize Hypotheses: Repeated assertive challenge plus CUS phrasing can stop unsafe action.
- Generate Solutions: Repeat concern, state safety issue explicitly, and prepare chain-of-command escalation if needed.
- Take Action: Use two-challenge communication, then escalate per policy when the risk remains unaddressed.
- Evaluate Outcomes: Unsafe step is paused/corrected and team expectations for speaking up are reinforced.
Related Concepts
- employee-engagement-skills-in-nursing-management - Engagement practices reduce recurrent conflict.
- leadership-styles-and-situational-use-in-nursing - Style choice affects conflict outcomes.
- management-functions-and-structures-in-nursing - Role clarity and process design prevent conflict triggers.
Self-Check
- Which conflict types most commonly threaten patient-safety communication?
- Why should root-cause analysis precede solution negotiation?
- What follow-up actions reduce repeat conflict episodes?