ISBAR Clinical Handoff Communication
Key Points
- ISBAR standardizes urgent and routine clinical communication across teams.
- The sequence is Introduction, Situation, Background, Assessment, Recommendation.
- Structured handoff reduces omission and supports faster shared understanding.
- ISBAR is useful for shift reports, interunit transfers, and escalation calls.
- Interprofessional updates should prioritize concise, clinically relevant language to reduce treatment delay.
- The mnemonic is easy to remember and keeps immediate-attention items visible during urgent communication.
- Adding readback (ISBARR) strengthens handoff reliability during high-risk transitions.
- ISBARR aligns with QSEN teamwork/collaboration competency and Joint Commission communication-focused patient-safety goals.
- I-PASS can be used as a complementary structure for interprofessional handoff, especially where explicit synthesis by receiver is expected.
- Bedside handoff with client inclusion improves continuity, safety, and nurse/client satisfaction when privacy safeguards are maintained.
- Inadequate handoff communication is a recognized severe-harm risk, so standardized structure and readback are core safety controls.
- Handoff is a real-time transfer and acceptance of care responsibility, not only a one-way information report.
- Transfer report should be destination-focused so the receiving team gets the most actionable data for that acuity level.
- Perioperative handoff should explicitly confirm patient-verified procedure/laterality, surgeon site marking, and allergy reaction profile to reduce wrong-site risk.
- In emergency-trauma pathways, combine EMS prearrival update with bedside ISBAR handoff to reduce setup and transfer omissions.
Equipment
- Up-to-date patient chart and current vital/lab trends
- Unit handoff template or ISBAR prompt card
- Escalation contact pathway for recommendation follow-through
Procedure Steps
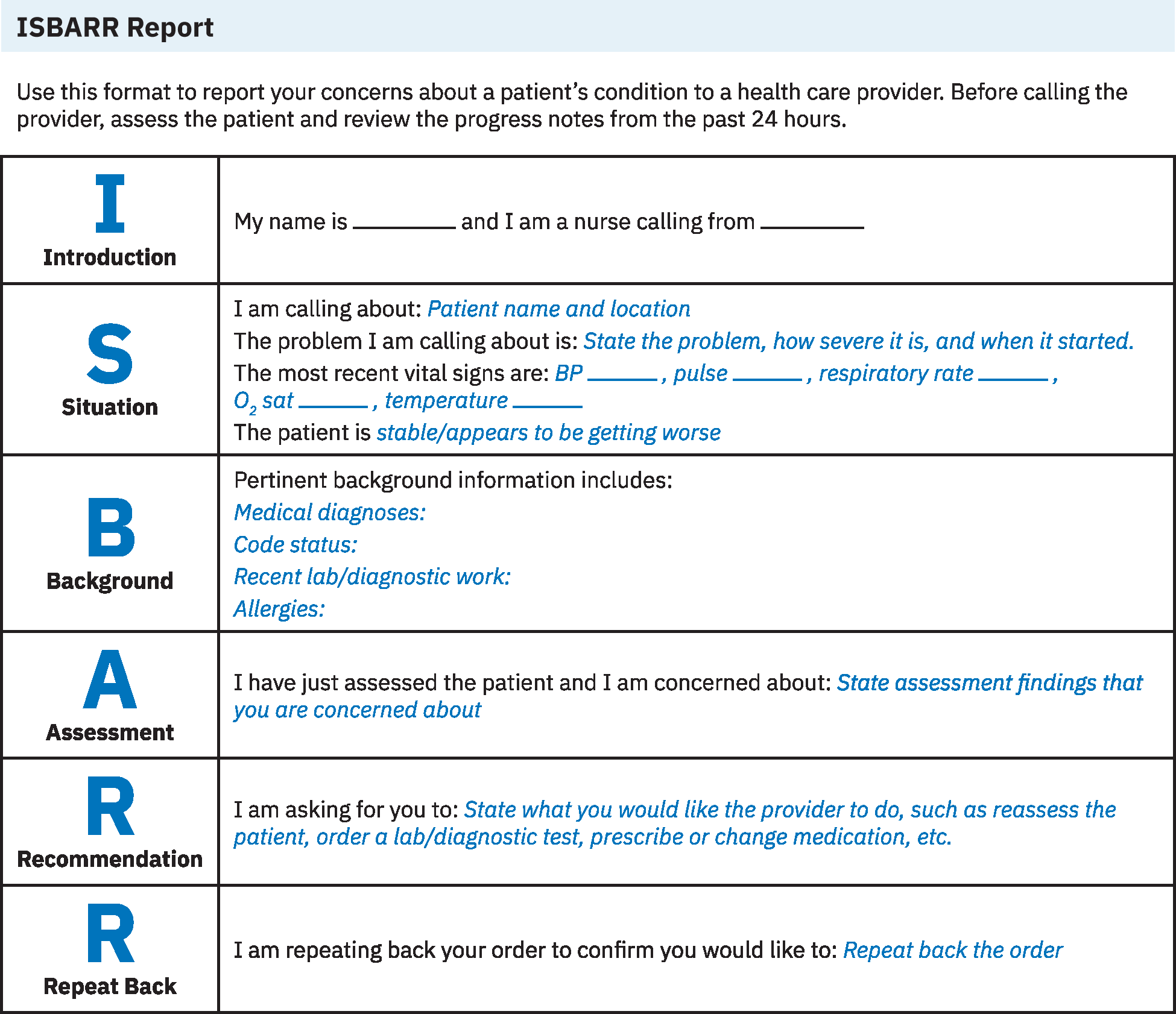 Illustration reference: OpenStax Fundamentals of Nursing Ch.8.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.8.2.
- Introduction: Identify yourself, role, unit, and patient identifiers.
- Situation: State the immediate reason for communication, urgency level, current status, and recent vital-sign trend.
- Background: Provide concise relevant history, admitting context, code status, allergies, recent interventions, and key lab/diagnostic findings.
- Assessment: Report current clinical interpretation using objective and subjective cues.
- Recommendation: Specify requested action, timeframe, and contingency if status worsens.
- Confirm transfer and acceptance of care responsibility and ask receiver to restate key plan elements.
- Add explicit readback confirmation for high-risk transfer details (code status, lines, wounds, pending tasks).
- For verbal provider orders, perform full closed-loop sequence: read back the order, execute the action, then state completion.
- Before escalation calls, complete pre-call preparation: direct patient assessment, current-order/protocol review, recent provider and nursing-note review, and charge-nurse consult when needed.
- Before calling, have high-yield data immediately available (admitting diagnosis/date, code status, allergies, recent vitals/labs, current medications/IV fluids, and active oxygen device/flow rate when used).
- During call planning, state your expected outcome/request clearly, then document who was contacted, exact call time, and summary of information shared/received immediately after the call.
- In admission-related handoff, explicitly identify present-on-admission findings (for example existing pressure injury or skin wound) and legal decision-maker status to avoid safety, documentation, and reimbursement errors.
- For interfacility transfer where charting systems differ, restate critical lines/drains/wounds/active therapies explicitly rather than assuming receiving-team EHR access.
- If your unit uses I-PASS, verify illness severity, patient summary, action list, situation awareness/contingency planning, and synthesis by receiver.
- For shift-to-shift bedside handoff, include the client, off-going nurse, and oncoming nurse in real time; include family only with client permission and HIPAA-safe setup.
- During bedside handoff assessment exchange, include baseline head-to-toe findings, current lines/tubes/drains, and recent changes in medications, labs, diagnostics, and treatments.
- During structured handoff, ensure minimum critical-content transfer: sender contact information, illness-severity framing, concise hospital-course summary, to-do list, contingency plans, allergies, code status, medication list, recent labs, and recent vital signs.
- Document handoff content, actions requested, and response timeline.
- For PACU-to-inpatient transfer, include minimum dataset elements: full identifiers (including medical ID), code status and allergies, procedure and anesthesia type/duration, current vital trend, IV medications/fluids and blood products, urine output, drain output, incision/dressing status, intraoperative complications, baseline versus current orientation/LOC, mobility restrictions, language/sensory support needs, family/decision-maker context, pending tests/procedures, and current low-hemoglobin or hemodynamic management plan.
- For interagency transfer, use receiving-facility checklist requirements and send expanded continuity details beyond unit-to-unit handoff minimums.
- For preop-to-OR transfer, verify with the patient and receiving nurse: full identifiers, procedure and laterality, consent alignment, surgeon-marked site, allergy band/reaction symptoms, and accompanying family-contact details when applicable.
- During PACU discharge or unit transfer calls, explicitly report readiness criteria status: vital-sign stability, effective pain control, return to baseline alertness/orientation, voiding status, and safe ambulation plan.
- In emergency-trauma intake, integrate prearrival EMS briefing into early ISBAR preparation, then complete a fuller secondary-survey handoff after stabilization.
- If definitive specialty services are unavailable locally (for example burn, stroke, or maternal-neonatal specialty care), use ISBAR to coordinate timely escalation and transfer to the appropriate facility.
Common Errors
- Giving unstructured narrative without recommendation → delayed action.
- Omitting key background risks → incomplete clinical context.
- Failing closed-loop confirmation → misunderstandings at transition points.
- Skipping synthesis by receiver → unverified plan and higher handoff error risk.
- No documentation of handoff and requests → weak accountability trail.
- Inadequate handoff can contribute to severe harm events (for example treatment delay, falls, medication errors, and wrong-site events).
Related
- continuity-of-care-during-evaluation-phase - ISBAR supports safe care transitions.
- ana-nursing-documentation-principles - Handoff quality depends on accurate source data.
- source-vs-problem-oriented-documentation-workflow - Documentation structure influences handoff clarity.
- leadership-attributes-and-competencies-in-nursing - Leadership behaviors drive reliable team communication during transitions.