Five Rights of Nursing Delegation
Key Points
- Delegation occurs when an RN asks LPN/LVN or assistive personnel to perform a task on the RN’s behalf.
- The RN remains accountable for the delegation decision and outcome.
- Safe delegation requires five rights: task, circumstance, person, communication, and supervision.
- Tasks requiring nursing judgment, independent teaching, or nursing care-plan decisions are not delegated to assistive roles.
- Unstable patients or unclear competencies require immediate RN reassessment.
- RN delegation decisions must also align with Nurse Practice Act, federal regulations, and agency policy.
- Safe delegation workflow includes assessment/planning, task-person selection, communication/resource setup, supervision/evaluation, and documentation/accountability.
- ANA Standard 5 (Implementation) and Standard 12 (Leadership) reinforce RN authority, ownership, accountability, and responsibility for delegation decisions.
- The nursing process itself is not delegated even when selected care elements are delegated.
- Delegation should remain respectful of both the delegatee and the patient.
- Nurse leaders should build a team climate where delegation requests are clear, safe, and professionally supported.
- Even when assistive personnel complete advanced training, high-impact tasks should be treated as delegated actions requiring RN validation and supervision.
- Right directions/communication includes what findings to collect, how to report, and by when; delegatees should not independently modify or re-delegate accepted tasks.
- Right supervision includes both direct observation and indirect outcome review, followed by constructive feedback and follow-up planning.
- Data collection may be delegated when appropriate (for example selected physical-exam data to LPN/LVN and vital-sign/weight measurement to UAP), but the RN remains responsible for data analysis and interpretation.
Pathophysiology
Delegation is a safety-critical workflow decision in dynamic care environments. Errors in delegation can create delayed treatment, omitted reassessment, or inappropriate task execution, increasing preventable adverse-event risk.
Classification
- Right task: Delegated activity is permitted by policy and delegatee role scope.
- Right circumstance: Patient is stable with predictable outcomes for delegated activity.
- Right person: Delegatee has verified competency and required training.
- Right communication: Instructions are clear, specific, and include opportunity for questions.
- Right supervision: RN monitors execution, verifies outcomes, and intervenes when needed.
- Regulatory-fit requirement: Delegation only proceeds when state/federal rules and institutional policy permit the task.
- Delegation workflow sequence: Assess and plan, select task/delegatee, communicate and provide resources, supervise and evaluate, then document and close accountability.
- Authority-accountability-responsibility triad: RN has authority to delegate, remains accountable for delegation decisions/outcomes, and retains responsibility for supervision and final care quality.
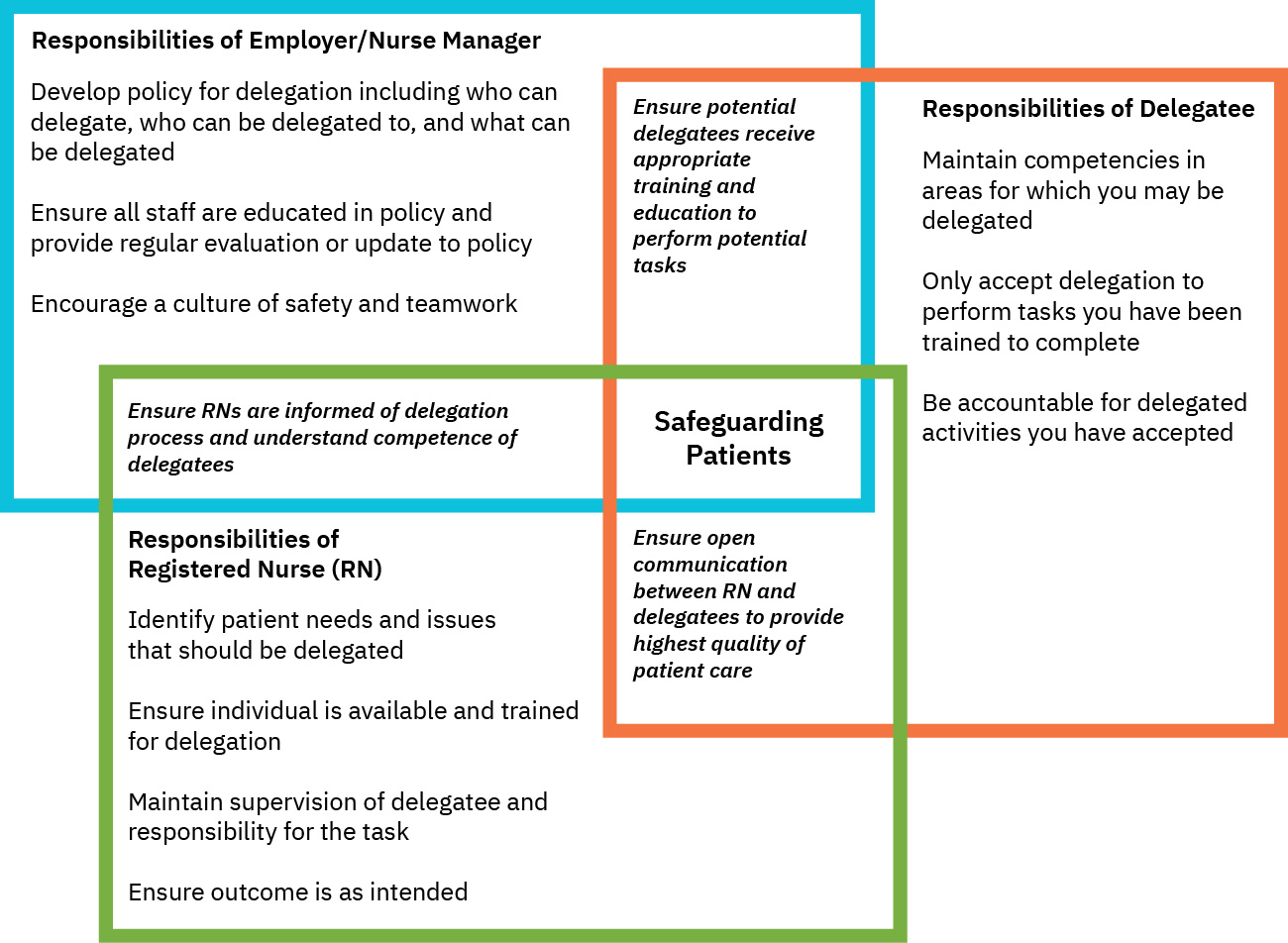 Illustration reference: OpenStax Fundamentals of Nursing Ch.15.5.
Illustration reference: OpenStax Fundamentals of Nursing Ch.15.5.
Nursing Assessment
NCLEX Focus
Before delegating, assess patient stability, delegatee competence, and your ability to supervise in real time.
- Confirm the task is policy-approved for the intended delegatee role.
- Reassess current patient condition for stability and expected trajectory.
- Verify delegatee education/check-offs for specialized skills.
- Exclude role-restricted work such as initial assessments, evaluation decisions, independent teaching, discharge decisions, and interpretation-heavy nursing judgment tasks.
- Determine whether communication pathway supports timely clarifications.
- Confirm delegatee acceptance of the task and reinforce that task modifications require RN consultation.
- Identify five-right breaches explicitly (task, person, circumstance, communication, supervision) before delegation proceeds.
- Ensure RN capacity for follow-up supervision and outcome validation.
Nursing Interventions
- Delegate only tasks that meet all five rights simultaneously.
- Provide concise, explicit directions, expected reporting thresholds, and closed-loop read-back when risk is high.
- Require immediate communication of unexpected findings.
- Perform RN verification for abnormal or high-risk results.
- Require delegatees to notify the RN immediately if they cannot complete the accepted delegated task so the RN can reassign or perform it.
- Use post-task constructive feedback prompts (correctness, outcome achievement, communication timeliness, challenges, and safety concerns) and define a follow-up support plan.
- In pressure-injury prevention, delegate routine turning/skin checks/moisture care only with explicit escalation triggers and RN follow-up.
- When UAP staff hold additional training (for example medications, injections, Foley care) verify policy allowance and competency each shift, then delegate with explicit RN oversight rather than assuming routine assignment status.
- If delegation safety is uncertain, perform the task directly rather than delegating under ambiguity.
- Document delegation rationale, instructions, supervision actions, and evaluation of delegated-task effectiveness.
- Include post-task follow-up feedback and a future delegation plan when performance gaps are identified.
- Require delegatees to maintain competency validation for delegated activities through ongoing check-offs/education per policy.
Accountability Reminder
Delegation transfers a task, not RN accountability for patient safety and care quality.
Pharmacology
Medication-related delegation must follow role limits, policy scope, and RN supervision requirements. In many settings, medication administration remains outside UAP scope, so role-policy verification is required before delegation.
Clinical Judgment Application
Clinical Scenario
An RN delegates a patient transfer to assistive personnel and later receives report of near-fall instability.
- Recognize Cues: Delegated mobility task now has altered safety context.
- Analyze Cues: Right circumstance may no longer be met.
- Prioritize Hypotheses: Patient instability requires RN reassessment before further delegation.
- Generate Solutions: Reclassify assistance level and adjust delegation plan.
- Take Action: Intervene directly and update team instructions.
- Evaluate Outcomes: Transfer proceeds safely with revised support.
Related Concepts
- nursing-diagnosis-and-collaborative-problems - Helps determine when RN-led versus delegated action is appropriate.
- medication-order-types-and-required-components - Supports safe role-based execution after order verification.
- isbar-clinical-handoff-communication - Structured communication framework that improves delegation clarity.
Self-Check
- Which patient factors can invalidate the right circumstance after delegation begins?
- Why does right person require competency verification, not assumption?
- What supervision actions are mandatory when delegated findings are abnormal?