Reproductive System
Key Points
- Reproductive function is hormone-regulated and involves both male and female organ systems.
- Puberty, menstrual cycling, and menopause reflect major female reproductive transitions.
- Menstrual flow commonly lasts about 3 to 5 days, and menopause often occurs in the late 40s to early 50s with vasomotor and mood symptoms.
- Aging male prostate enlargement can impair urination and increase infection risk.
- Menstrual-cycle tracking is counted from the first day of bleeding to the first day of the next cycle, and intermenstrual bleeding is abnormal.
- Early pubertal activation reflects increasing GnRH-LH/FSH signaling, often beginning with nocturnal LH rise before visible secondary sex changes.
- The vulva protects the urethral opening and vaginal introitus, and the clitoris includes both external and internal erectile structures.
- In typical AFAB pubertal progression, thelarche often appears first (around ages 9 to 10), followed by pubarche and then menarche.
- In aging males, testosterone production may decline (andropause/late-onset hypogonadal pattern), with possible lower libido, mood change, and fat-redistribution symptoms.
Pathophysiology
The reproductive system supports gamete production, fertilization potential, and sex-hormone influenced body changes. Endocrine signaling regulates development, sexual function, and reproductive timing across the lifespan, and also influences appetite, mood, temperature regulation, and stress response.
In females, cyclic ovarian hormone changes drive ovulation and menstruation until menopause. In males, testosterone supports secondary sex traits and sperm production, while age-related prostate enlargement can obstruct urinary outflow.
Male endocrine regulation follows the hypothalamic-pituitary-gonadal axis: hypothalamic GnRH stimulates pituitary LH/FSH release, LH supports testicular testosterone production, and testosterone exerts negative feedback on hypothalamic-pituitary signaling. Testosterone contributes to secondary sex characteristics such as body-hair distribution, voice deepening, heavier bone structure, increased hematocrit tendency, and typical male-pattern fat distribution.
Menstrual cycling typically includes ovulation about monthly and menstruation when fertilization does not occur. Menopause follows estrogen decline and may present with irregular periods, hot flashes, night sweats, mood shifts, and metabolic change. Cycle physiology integrates ovarian follicular/luteal phases with uterine proliferative/secretory phases; menstrual bleeding commonly lasts about 3 to 7 days with average blood loss around 30 to 40 mL. In a typical 28-day pattern, follicular activity dominates the first half of the cycle, ovulation commonly occurs around mid-cycle, and the luteal phase lasts about 14 days with progesterone-supported endometrial thickening.
Ovarian-cycle coordination includes follicular growth under FSH, rising estrogen from the dominant follicle, and an LH surge that triggers ovulation. Tubal cilia and muscular contractions then support transport of the oocyte or early embryo toward the uterine cavity.
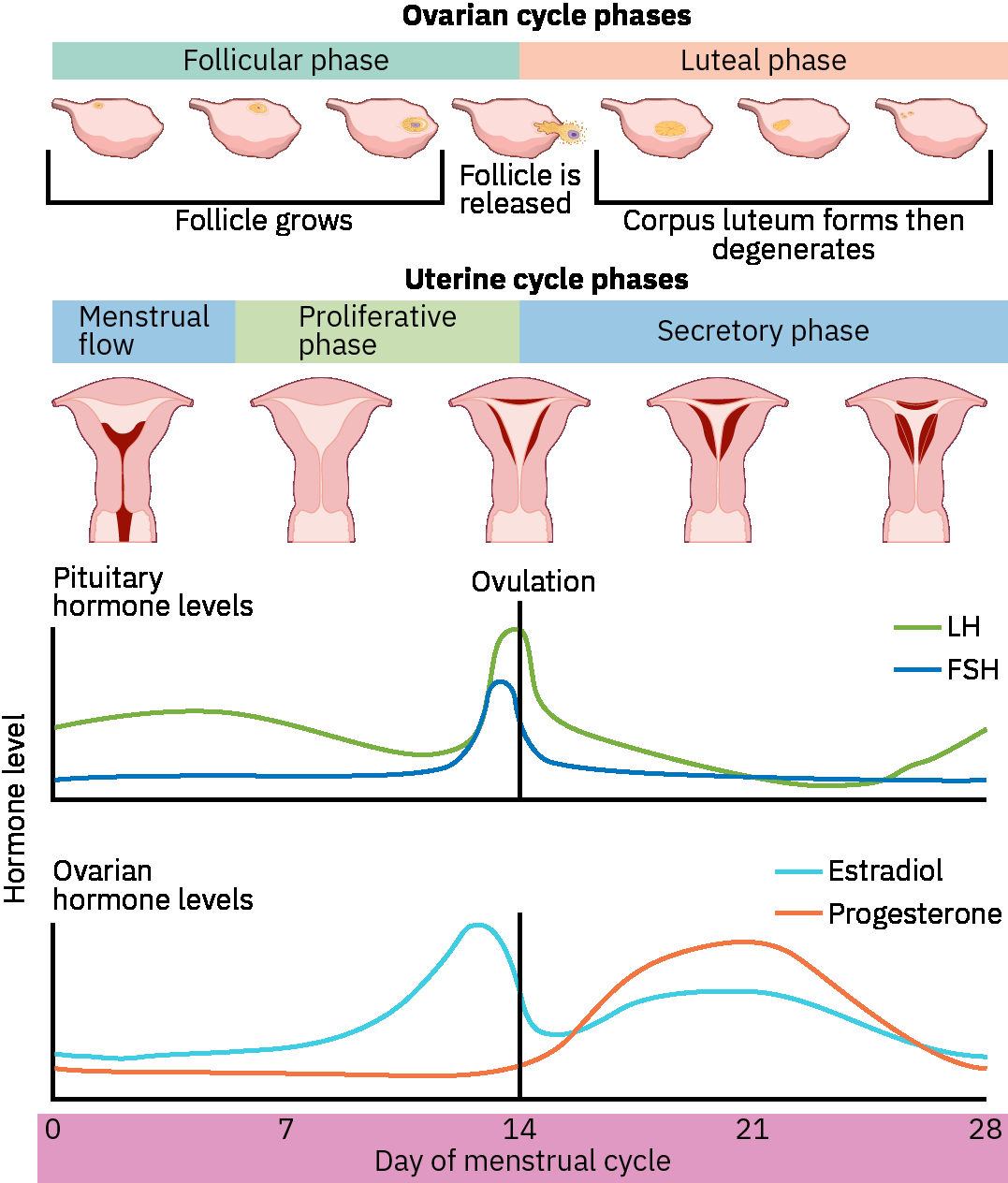 Illustration reference: OpenStax Pharmacology Ch.36.1.
Illustration reference: OpenStax Pharmacology Ch.36.1.
With aging, male sexual response may become slower and less intense, but fertility can persist into older adulthood. In female aging, hypoestrogenic changes can cause vaginal dryness, dyspareunia, urinary urgency/frequency, recurrent UTI risk, reduced pelvic-floor tone, and prolapse risk.
Male reproductive function depends on coordinated endocrine and ductal activity: testes produce both sperm and testosterone, the epididymis supports sperm maturation and storage, and accessory glands (seminal vesicles, prostate, and bulbourethral glands) add fluid components that support sperm transport and ejaculation. Seminal-vesicle fructose supports sperm energy needs, and prostatic alkaline fluid helps initial semen coagulation followed by liquefaction to support forward sperm movement. Spermatic-cord structures connect the testes to abdominal structures through the inguinal canal and are clinically relevant in torsion, hernia, and varicocele presentations.
The penile urethra provides a shared passageway for urine and semen. During sexual arousal and ejaculation phases, urine flow through this pathway is functionally inhibited, so urine and semen are not expelled simultaneously.
The testes remain in the scrotum, where temperature is typically lower than core body temperature, supporting efficient spermatogenesis. Sperm mature in the epididymis, then travel through the vas deferens toward seminal-vesicle and prostatic secretions before ejaculation through the urethral route. Bulbourethral glands provide pre-ejaculatory lubrication that supports urethral transit.
Female internal anatomy includes a muscular vagina, uterus/cervix, ovaries, and fallopian tubes with fimbriae. Vaginal normal flora (especially lactobacillus) help maintain acidic pH (about 3.8 to 4.5) and infection protection; douching disrupts this protective environment. Uterine layers include perimetrium, myometrium, and endometrium, with the endometrium serving as the implantation site or shedding during menstruation.
External genital anatomy includes the mons pubis, labia majora, labia minora, and clitoris. The clitoris has both external and internal portions, and vulvar structures protect the urethral opening and vaginal introitus while supporting sexual function and comfort.
The female urethra is shorter than the male urethra (often around 3 to 4 cm) and has a separate external opening from the vaginal introitus, so urinary and reproductive outflow occur through different openings.
Classification
- Female reproductive components: Vulva (mons pubis, labia majora/minora, clitoris, vestibule, Bartholin glands, and perineum), vaginal and urethral openings, vagina, uterus/cervix, fallopian tubes, and ovaries.
- External-landmark orientation: Urethral opening lies below the clitoral hood and above the vaginal introitus, supporting accurate assessment and trauma-aware perineal care.
- Female structural-functional landmarks: Cervix as uterine outflow/inflow gateway, fundus as pregnancy-growth landmark, and tubal ampulla as common fertilization site.
- Fallopian-tube segments: Infundibulum and fimbriae capture the oocyte, ampulla supports typical fertilization location, and isthmus connects toward the uterine cavity.
- Male reproductive components: Penis, scrotum, testes, seminiferous tubules, epididymis, spermatic cord, vas deferens, and accessory glands (seminal vesicles, prostate, bulbourethral glands).
- Male reproductive risk conditions: Cryptorchidism, testicular torsion, inguinal hernia extension into the scrotum, and varicocele-associated fertility impact.
- Lifecycle transitions: Puberty onset, cyclical menstruation/ovulation, and menopause.
- Pubertal-development tracking: Secondary sex characteristics progress through Tanner stages from prepubertal to mature patterns.
- Puberty sequence landmarks (AFAB): Thelarche often begins around ages 9 to 10, pubarche commonly follows within about 6 months, menarche often occurs about 1 to 3 years after thelarche (average around 12.8), and first ovulation may follow within about 6 to 9 months.
- Cycle-regulation landmarks: Estrogen-predominant phases soften the cervix and increase clear/stretchy mucus, while progesterone-dominant phases support cervical integrity and reduced sperm passage.
- Aging-related changes: Prostate enlargement with urinary-flow impact in older males.
- Male aging-hormone transition: Some clients experience andropause-pattern decline in testosterone with variable mood, libido, and body-composition effects.
- Menopause transition criteria: Clinical menopause is defined by 12 months without menses (often with elevated FSH); postmenopausal bleeding is abnormal and requires evaluation.
Nursing Assessment
NCLEX Focus
Priority questions emphasize identifying age-related reproductive changes that increase urinary or infection risk.
- Observe for urinary hesitancy, weak stream, retention, and frequency changes in older male clients.
- Assess for possible late-onset hypogonadal symptom patterns in aging males (decreased libido, depressed mood, and fat redistribution) and escalate for medical evaluation when function declines.
- Assess cancer-related urinary pattern change (frequency, urgency, scant output) and pain burden in male clients with suspected or known prostate disease.
- Report signs of urinary infection promptly when retention or incomplete emptying is suspected.
- Assess comfort, hygiene needs, and privacy preferences in all personal care interactions.
- Use respectful language and preserve dignity during reproductive-system related care.
- Confirm affirmed identity and communication preferences while collecting clinically relevant sex-assigned-at-birth context when needed for safe assessment pathways.
- Escalate sudden severe scrotal pain or swelling immediately because interrupted testicular blood flow can rapidly threaten tissue viability.
- Treat persistent erection lasting 4 hours or longer as an emergency cue requiring immediate escalation.
- Recognize normal anatomic variation in external genital appearance and avoid pathologizing expected differences in size, shape, or pigmentation.
- Escalate abnormal menstrual patterns such as prolonged bleeding beyond expected duration, very heavy volume, or bleeding between cycles.
- Escalate any vaginal bleeding occurring more than 12 months after the final menstrual period.
Nursing Interventions
- Support perineal hygiene and hydration habits that reduce infection risk.
- Reinforce avoidance of douching and other practices that disrupt protective vaginal flora.
- Encourage timely reporting of urinary changes in clients with known prostate symptoms.
- Reinforce treatment-expectation education for prostate radiation therapy, including fatigue, local skin irritation, and potential urinary symptom flare.
- Maintain person-centered privacy and trauma-informed communication during care.
- Use nonjudgmental, inclusive communication in all reproductive-health encounters and avoid assumptions about identity or anatomy.
- Reinforce routine health follow-up and preventive education as directed.
- Treat suspected testicular torsion as a time-sensitive emergency and prioritize immediate provider notification.
- Escalate suspected priapism urgently to reduce risk of permanent erectile dysfunction.
- Teach menopause symptom self-management (layered clothing, sleep hygiene, vaginal moisturizers/lubricants) and when to seek medical evaluation.
Retention-Related Infection Risk
Persistent urinary retention can quickly increase UTI risk and requires prompt nurse notification.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| alpha-blockers | BPH-management context | Monitor symptom trends and report persistent voiding difficulty. |
| antibiotics | UTI-treatment context | Escalate worsening urinary symptoms or systemic signs despite treatment. |
Clinical Judgment Application
Clinical Scenario
An older male resident reports frequent urgency, weak urinary stream, and new suprapubic discomfort.
- Recognize Cues: Obstructive voiding pattern with possible retention complications.
- Analyze Cues: Prostate enlargement may be reducing bladder emptying and increasing infection risk.
- Prioritize Hypotheses: Immediate priority is early escalation before retention worsens.
- Generate Solutions: Report findings, monitor output pattern, and support hydration/toileting assistance.
- Take Action: Implement comfort/safety supports while nurse evaluates.
- Evaluate Outcomes: Symptoms are addressed and infection/retention complications are prevented.
Related Concepts
- urinary-system - Urinary function overlap is central in prostate-related changes.
- urinary-tract-infections - Incomplete emptying elevates infection risk.
- endocrine-system - Hormonal regulation drives reproductive maturation and transition.
- postpartum-hemorrhage - Reproductive-system recovery is a major postpartum focus.
- therapeutic-communication - Respectful communication preserves dignity in sensitive-care contexts.
Self-Check
- Which urinary findings suggest prostate-related obstruction in older adults?
- How does endocrine signaling shape reproductive changes across the lifespan?
- Which caregiver behaviors best protect dignity during reproductive-related care?