Physiologic Changes during the Postpartum Period
Key Points
- The postpartum period (often called the fourth trimester) lasts about 6 weeks and includes rapid immediate changes plus gradual systemic recovery.
- Key trends include uterine involution, lochia transition, diuresis/diaphoresis, and shifting hemodynamics.
- In the first 5 to 7 postpartum days, about 2 liters of excess extracellular fluid are commonly eliminated; edema may persist longer after large intrapartum IV-fluid exposure.
- Early postpartum urinary output can be very high (up to about 3,000 mL in 24 hours), but retention/overdistention still requires prompt intervention to protect uterine involution.
- Early recognition of abnormal vitals, bleeding, infection signs, and urinary retention prevents major complications.
Pathophysiology
After birth, endocrine withdrawal and placental separation trigger rapid cardiovascular, fluid, reproductive, and metabolic adjustments. Immediate postpartum shifts include increased intravascular return, brisk diuresis/diaphoresis, uterine contraction for hemostasis, and initiation of lactation pathways. Blood pressure and cardiac output are commonly elevated for about the first 48 hours because extracellular fluid moves back into the intravascular space and transiently increases preload.
Recovery then progresses over weeks as organs move toward prepregnant state. The uterus involutes approximately 1 cm per day in early postpartum, is expected near the umbilicus in the first 24 to 48 hours, and approaches the suprapubic level by about Day 10. Lochia transitions from rubra to serosa to alba as placental-site healing advances. Cervical dilation generally contracts to under 1 cm by about Day 7, while cervical-os shape may remain a transverse slit after vaginal birth.
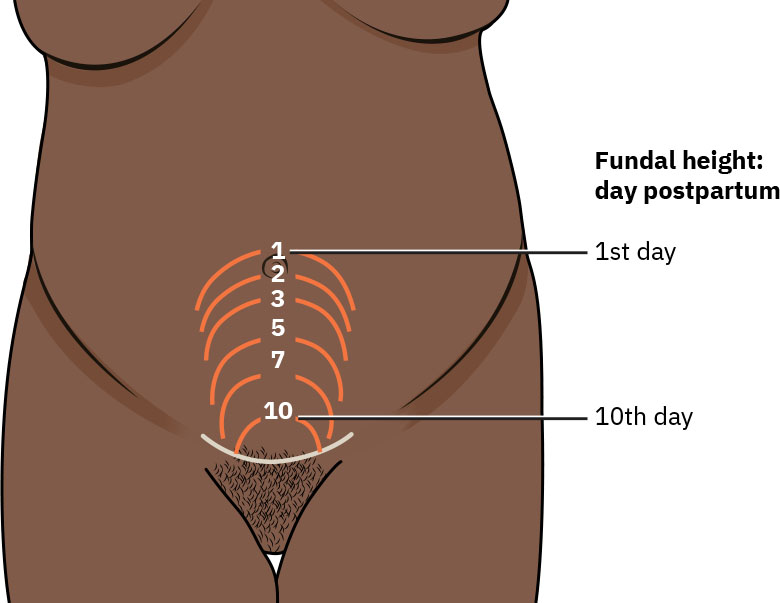 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.20.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.20.1.
Expected birth blood loss spans a broad physiologic range (commonly around 150 to 1000 mL across vaginal and cesarean birth contexts), and residual placental blood volume can contribute additional measurable postpartum blood loss. This baseline overlap requires trend-focused assessment rather than one-time visual estimation.
Vaginal and perineal tissue can remain swollen after birth, and laceration/episiotomy repairs commonly require roughly 2 to 3 weeks for healing. Pelvic-floor tone often decreases transiently after birth, contributing to stress urinary leakage that can improve with targeted pelvic-floor exercises.
Lactation physiology also evolves rapidly: colostrum is present at birth, transitional milk commonly increases around postpartum day 2 to 3, and mature milk is usually established by about 2 weeks.
Musculoskeletal recovery includes short-term fatigue/body aches from labor, gradual reduction of pregnancy-related pelvic laxity, and progressive core-strength return. Pregnancy hormone effects (including relaxin-mediated ligament softening) can leave temporary pelvic instability, lordosis-related discomfort, and altered center of gravity that improve gradually over the postpartum months. If diastasis recti remains wider than about 2 cm at 6 weeks postpartum, evaluation and physical-therapy referral are appropriate. Integumentary changes such as linea nigra and generalized hyperpigmentation usually fade, while striae often lighten but do not fully disappear.
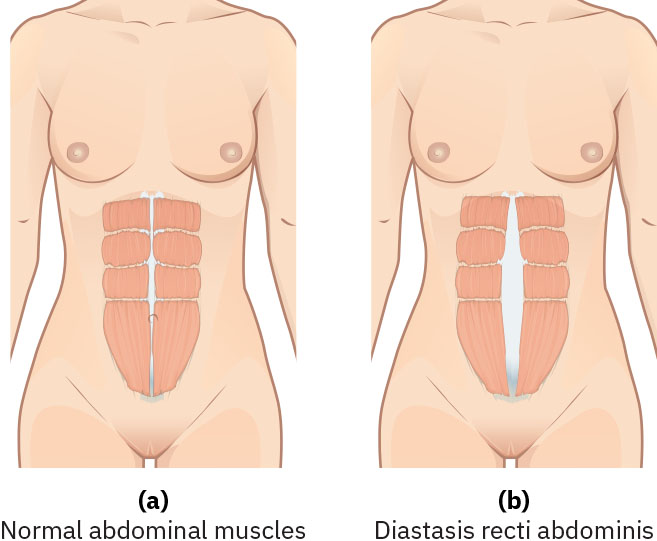 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.20.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.20.1.
Gastrointestinal recovery can include transient nausea, delayed bowel motility (more pronounced after cesarean birth), and constipation related to dehydration, reduced intake, analgesics/anesthetics, and perineal discomfort. Passing flatus is an early sign of bowel-motility return, and routine bowel movements commonly resume within about 2 to 3 days postpartum.
Nutrition recovery typically includes immediate postpartum weight loss (about 10 to 15 lb from delivery products), then gradual reduction of remaining pregnancy weight. Lactating patients generally need additional daily calories (about +330 kcal/day during the first 6 months, then about +400 kcal/day after 6 months when prepregnancy weight has returned).
Neurologic adaptation after neuraxial anesthesia may include transient lower-extremity sensory symptoms, but severe postural headache that worsens when sitting up raises concern for dural-puncture headache. Persistent headache despite position change, especially with elevated blood pressure or visual/epigastric symptoms, requires urgent evaluation for postpartum preeclampsia; eclamptic-seizure risk can persist for up to 6 weeks postpartum.
Hematologic patterns also shift postpartum: stress leukocytosis can reach about 20,000 to 30,000 cells/microL and may persist for several days before returning toward prepregnant levels within about 1 week; platelet nadir often occurs on postpartum day 1 before recovery; fibrinogen and erythrocyte sedimentation rate can remain elevated during early recovery. Postpartum anemia is common after delivery blood loss; many guidelines use hemoglobin below 10 g/dL at or beyond 48 hours postpartum as an operational threshold for evaluation and treatment planning.
Classification
- Immediate physiologic changes (first 24 hours): Hemodynamic/fluid shifts, early involution, and acute bleeding surveillance.
- Early postpartum changes (days 1 to 10): Continued involution, lochia evolution, bladder/bowel recovery, breast changes.
- Extended postpartum changes (up to 6 weeks): Ongoing uterine recovery, tissue healing, and functional adaptation.
- Delayed recovery pattern: Subinvolution (inadequate uterine return toward prepregnant size), often linked to retained tissue or uterine infection risk.
- Involution-inhibiting factors: Prolonged labor, multiple gestation/birth, retained placental tissue, and persistent bladder overdistention.
Nursing Assessment
NCLEX Focus
Priority items test expected-versus-abnormal postpartum findings and first interventions for hemorrhage-risk cues.
- Assess temperature, blood pressure, pulse, and oxygenation trends; report persistent abnormal patterns promptly.
- Interpret early postpartum trends in context: brief temperature rise can occur in first 24 hours (dehydration/work of labor), but persistent fever above 38 C suggests infection; postpartum bradycardia (about 50 to 70/min) can persist for 6 to 10 days, while HR above 100 warrants escalation.
- Compare postpartum blood pressure with baseline: around 130/80 mm Hg can be seen in immediate recovery with pain/anxiety, but BP above 140/90 with headache/visual symptoms suggests postpartum preeclampsia and BP below 90/60 with dizziness/weakness/tachycardia suggests hypovolemia.
- Monitor for fluid-overload warning signs in higher-risk patients (worsening dyspnea, tachycardia, crackles, pink-tinged frothy sputum, or hypoxemia).
- Assess fundus for firmness, height, and midline position; evaluate lochia amount/color/odor.
- Differentiate expected lochia timeline (rubra about Days 1 to 4, serosa about Days 4 to 10, alba about Days 10 to 28) from abnormal persistence or reversal to heavier red bleeding.
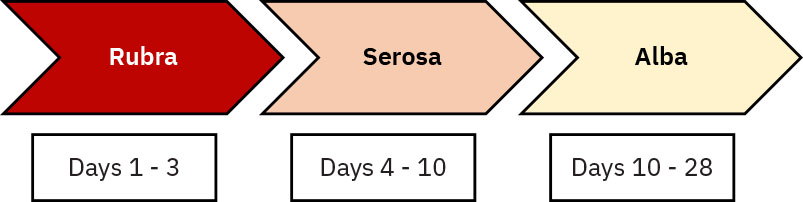 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.20.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.20.1.
- Screen for bladder distention, retention, and bowel recovery barriers.
- Bladder overdistention cues include suprapubic fullness, frequent small voids (for example, less than 150 mL), discomfort, unexpectedly high fundal position, lateral fundal deviation, boggy tone, or increased lochia.
- Recognize retention drivers in immediate postpartum: periurethral edema after vaginal birth, perineal pain after laceration/episiotomy repair, and delayed voiding sensation after epidural or spinal anesthesia.
- Assess bowel-function return (especially after cesarean birth), constipation burden, and readiness for diet advancement as motility recovers.
- Evaluate pain, breast/lactation adaptation, and signs of infection or delayed involution.
- Distinguish expected post-neuraxial discomfort from concerning neurologic signs (persistent severe headache, visual change, photophobia, hyperreflexia, or worsening hypertension).
- Trend postpartum CBC/coagulation results with symptoms (fatigue, dizziness, dyspnea, palpitations, infection cues, unilateral-leg DVT signs) and escalate abnormal patterns promptly.
Nursing Interventions
- Perform fundal support/massage when indicated and reassess bleeding response.
- Promote frequent voiding and catheterization per protocol if retention persists.
- Use structured provider handoff (for example SBAR) when escalating abnormal temperature, BP, pulse, or bleeding trends.
- Provide education on expected lochia progression and warning signs (heavy bleeding, foul odor, large clots).
- Teach that afterpains are usually strongest in the immediate hours after birth and can continue for about 2 to 3 days, often more noticeable in multiparous patients and during breastfeeding.
- Offer afterpain comfort measures (for example side-lying with fundal splint support, warm compress/heating pad, and prescribed NSAID pathways when appropriate).
- Support lactation or suppression goals with individualized teaching and comfort measures.
- Support bowel recovery with early ambulation, hydration, fiber-forward intake, and prescribed stool-softener/laxative pathways when indicated.
Postpartum Hemorrhage Risk
A boggy or displaced fundus with heavy lochia requires immediate correction and escalation to prevent rapid decompensation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| uterotonics | Oxytocin postpartum context | Maintains uterine tone and reduces hemorrhage risk during early recovery. |
| nsaids | Postpartum cramping-pain context | Helps control afterpains while preserving function and feeding participation. |
Clinical Judgment Application
Clinical Scenario
A postpartum patient reports heavy bleeding; assessment reveals a firm but right-deviated fundus and palpable bladder fullness.
- Recognize Cues: Increased lochia with uterine deviation and retention indicators.
- Analyze Cues: Bladder distention is likely impairing effective uterine positioning and tone dynamics.
- Prioritize Hypotheses: Immediate priority is restoring uterine alignment and preventing hemorrhage progression.
- Generate Solutions: Assist voiding/catheterize per protocol, reassess fundus/lochia, and monitor vitals.
- Take Action: Implement bladder-emptying and repeat focused postpartum assessment.
- Evaluate Outcomes: Fundus returns midline and bleeding decreases to expected postpartum range.
Related Concepts
- nursing-care-during-the-fourth-stage-of-labor - Immediate postpartum surveillance begins here.
- complications-in-the-third-stage-of-labor - Early postpartum trends may reflect unresolved third-stage issues.
- postpartum-hemorrhage - Critical complication linked to tone, placental factors, and delayed response.
- breasts-and-breast-feeding - Early lactation supports neonatal nutrition and maternal adaptation.
- psychosocial-adaptation-to-parenthood - Physiologic recovery intersects with emotional transition.
Self-Check
- What lochia pattern is expected across rubra, serosa, and alba stages?
- Why can bladder distention worsen postpartum bleeding risk?
- Which vital-sign combinations in postpartum assessment should trigger urgent escalation?