Nursing Care during the Fourth Stage of Labor
Key Points
- Fourth stage spans about 1 to 4 hours after placental birth and requires intensive monitoring.
- Priority surveillance includes vital signs, fundal tone/location, lochia, bladder status, and pain.
- Early parent-newborn bonding and feeding support occur alongside ongoing hemorrhage prevention.
Pathophysiology
The fourth stage is the immediate postpartum stabilization period when uterine involution and hemostatic control must remain effective after major circulatory and hormonal shifts. During this window, the risk of uterine atony and postpartum hemorrhage remains significant. This stage also includes immediate postbirth repair and mobility transition needs, so close skilled attendance is required while maternal-newborn recovery is established.
Physiologic recovery occurs concurrently with emotional transition and newborn adaptation. Nursing care therefore combines rigorous safety surveillance with supportive attachment and education.
Classification
- Physiologic surveillance domain: Vital-sign trend, fundal assessment, lochia progression, and bladder effects on uterine tone.
- Complication domain: Uterine atony, concealed or overt hemorrhage, hematoma, and delayed recovery signs.
- Recovery-support domain: Pain management, mobility assistance, and emotional reassurance.
- Bonding/feeding domain: Skin-to-skin facilitation and early breastfeeding support.
Nursing Assessment
NCLEX Focus
Priority questions test which postpartum finding signals early hemorrhage and which intervention should occur immediately.
- Obtain vital signs every 15 minutes in the first hour and every 30 minutes in the second hour, then hourly thereafter until postpartum transfer (or per agency protocol).
- Assess fundus for firmness, midline position, and expected involution trend.
- In immediate recovery, expect fundus near the umbilicus and escalate if fundal height rises in early hours instead of remaining stable/downtrending.
- Assess lochia amount/color/consistency and quantify blood loss when indicated.
- Use quantitative blood loss methods (measuring and weighing blood-soaked materials) when bleeding concern is present.
- For weighted lochia methods, use the 1 g to 1 mL conversion and keep cumulative postpartum totals with delivery QBL.
- Evaluate bladder distention, perineal status, pain level, and emotional response.
- Evaluate parent-newborn and support-person-newborn interaction quality (holding, touching, and responsive engagement) and escalate persistent disengagement concerns.
- Watch for hypotension, fever development, and ambulation limitations related to blood loss, perineal trauma, fatigue, or recent neuraxial anesthesia.
- Recognize expected lochia rubra as dark-to-bright red discharge with possible small clots while escalating excessive bleeding patterns.
- Escalate for lochia clots larger than about a quarter, foul odor, or pad saturation within an hour.
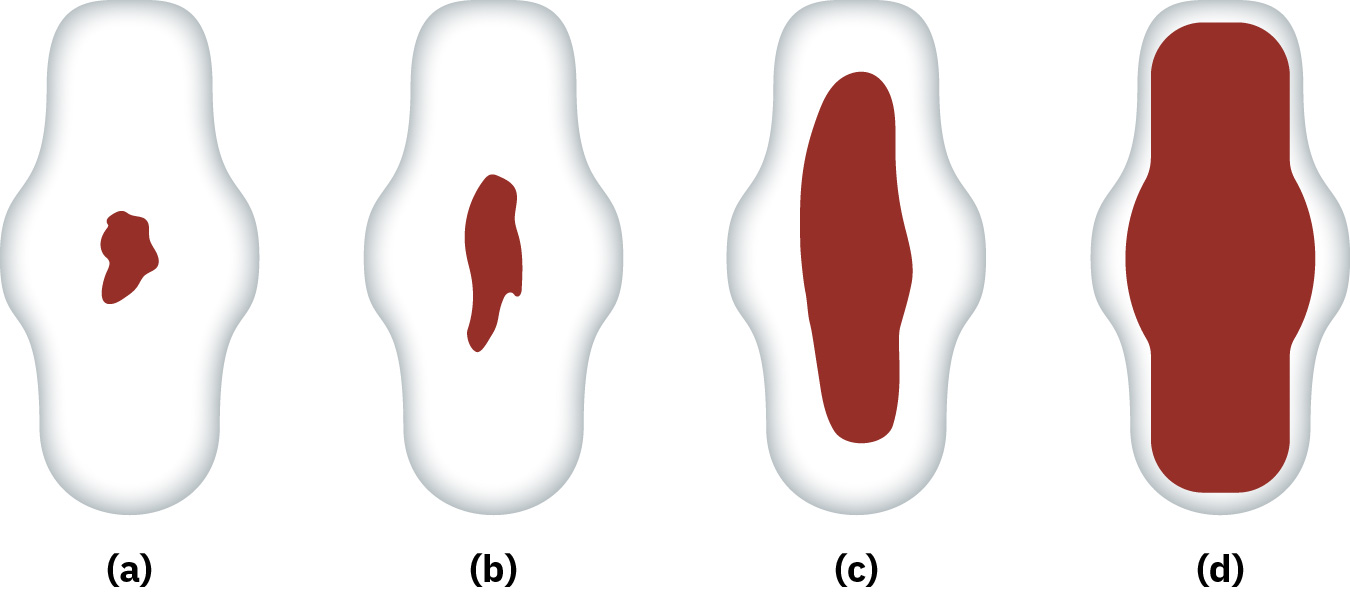 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.18.4.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.18.4.
- During fundal assessment, treat persistent blood streaming or large expressed clots as urgent escalation cues for hemorrhage pathway review.
- Assess perineal laceration-related pain/edema and screen severe pain or marked bruising for possible hematoma.
- Screen for decreased bladder sensation after birth and schedule void attempts until normal urge sensation returns.
- Monitor urine output and bladder distention closely after neuraxial anesthesia because retention can worsen uterine atony risk.
- During neuraxial recovery, reassess lower-extremity sensation/movement frequently before unassisted ambulation.
- Review bowel-function anxiety and constipation risk (especially severe tears, hemorrhoids, cesarean recovery, or opioid use).
Nursing Interventions
- Perform fundal massage when indicated and reinforce patient education about its purpose.
- Explain why repeated fundal checks/massage are needed to lower hemorrhage risk and improve patient acceptance of an uncomfortable intervention.
- Assist early voiding to reduce bladder-related uterine displacement and atony risk.
- Escalate promptly for heavy lochia, boggy fundus, or unstable vital signs.
- Use perineal comfort bundle as indicated (ice/heat, topical support, peri-bottle dilution during urination, rest, anti-inflammatory options, and sitz-bath education).
- Promote skin-to-skin contact, breastfeeding initiation, and family-centered reassurance.
- Teach early skin-to-skin benefits in concrete terms (newborn temperature/cardiorespiratory support, calming, feeding readiness, and maternal oxytocin support).
- For immediate post-cesarean recovery, include anesthesia recovery checks, urine output/catheter patency, and IV-site patency in the early surveillance bundle.
- Maintain thermal support conditions (warm room, dry infant blankets, and head covering when needed) while immediate adaptation continues.
- When maternal-newborn stability allows, protect uninterrupted skin-to-skin and breastfeeding initiation windows before routine weighing/measuring/newborn medication tasks.
- After epidural discontinuation, perform first-ambulation fall-risk support with assisted mobilization.
- Ask and document culturally grounded privacy preferences (for example provider/staff gender requests) and coordinate feasible accommodations with the care team.
Immediate Postpartum Hemorrhage Risk
A boggy or displaced fundus with increasing lochia can indicate impending or active hemorrhage and requires urgent correction and provider notification.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| uterotonics | Oxytocin, misoprostol, methylergonovine, carboprost context | Support uterine tone when bleeding risk or atony findings are present. |
| antifibrinolytics | Tranexamic acid context | Used in postpartum-hemorrhage (postpartum hemorrhage) pathways to reduce ongoing blood loss. |
Clinical Judgment Application
Clinical Scenario
Thirty minutes after placental delivery, a patient develops increased lochia and a soft fundus deviated from midline.
- Recognize Cues: Increased bleeding, boggy uterus, and possible bladder-related displacement.
- Analyze Cues: Findings suggest inadequate uterine contraction with rising hemorrhage risk.
- Prioritize Hypotheses: Immediate priority is correction of uterine atony and prevention of further blood loss.
- Generate Solutions: Fundal support, bladder management, rapid reassessment, and hemorrhage protocol communication.
- Take Action: Implement interventions and notify provider with objective trend data.
- Evaluate Outcomes: Fundus becomes firm/midline and bleeding decreases to expected range.
Related Concepts
- nursing-care-during-the-third-stage-of-labor - Third-stage events strongly influence fourth-stage risk profile.
- postpartum-hemorrhage - Key emergency to detect early in the immediate postpartum period.
- physiologic-changes-during-the-postpartum-period - Fundal trend assessment reflects recovery progression.
- postpartum-bonding - Emotional adaptation and attachment support begin in fourth stage.
- breasts-and-breast-feeding - Early latch support improves feeding success and maternal confidence.
Self-Check
- Which fourth-stage findings indicate routine recovery versus early hemorrhage?
- Why can bladder distention increase postpartum bleeding risk?
- Which education points improve patient cooperation with frequent fundal assessment?