Urinary Elimination Devices and Catheter Types
Key Points
- Urinary catheterization supports elimination when spontaneous bladder emptying is impaired or unsafe.
- Indwelling catheters use a retention balloon and continuous closed drainage.
- Catheter diameter is described by French size, with larger number indicating larger diameter.
- Collection-bag placement and tubing integrity directly affect backflow risk, urethral traction, and CAUTI risk.
Pathophysiology
Alternative urinary-elimination devices are used when normal voiding is disrupted by acute illness, surgery, obstruction, neurologic impairment, or functional limitations. Device misuse can increase urinary stasis, contamination, urethral trauma, and infection risk.
Closed drainage and gravity-dependent flow reduce reflux of contaminated urine into the bladder. Safe outcomes depend on maintaining unobstructed tubing and stable securement throughout mobility and repositioning.
Classification
- Indwelling catheter (Foley): Balloon-retained bladder catheter for continuous drainage through a closed collection system.
- insertion sizing principle: use the smallest effective diameter (commonly about 14 Fr in many adult workflows) unless clinical context requires otherwise
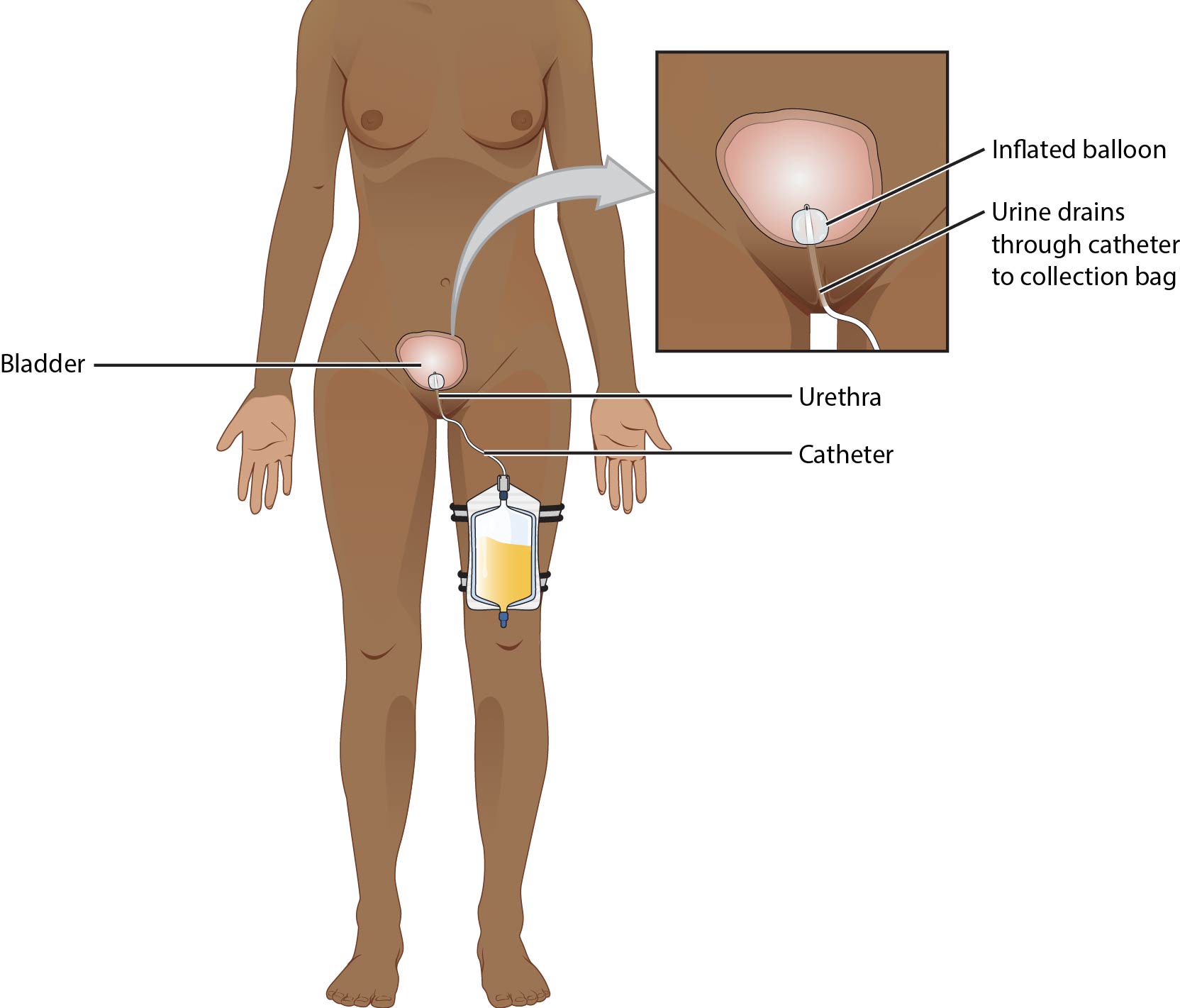 Illustration reference: OpenStax Clinical Nursing Skills Ch.19.4.
Illustration reference: OpenStax Clinical Nursing Skills Ch.19.4.
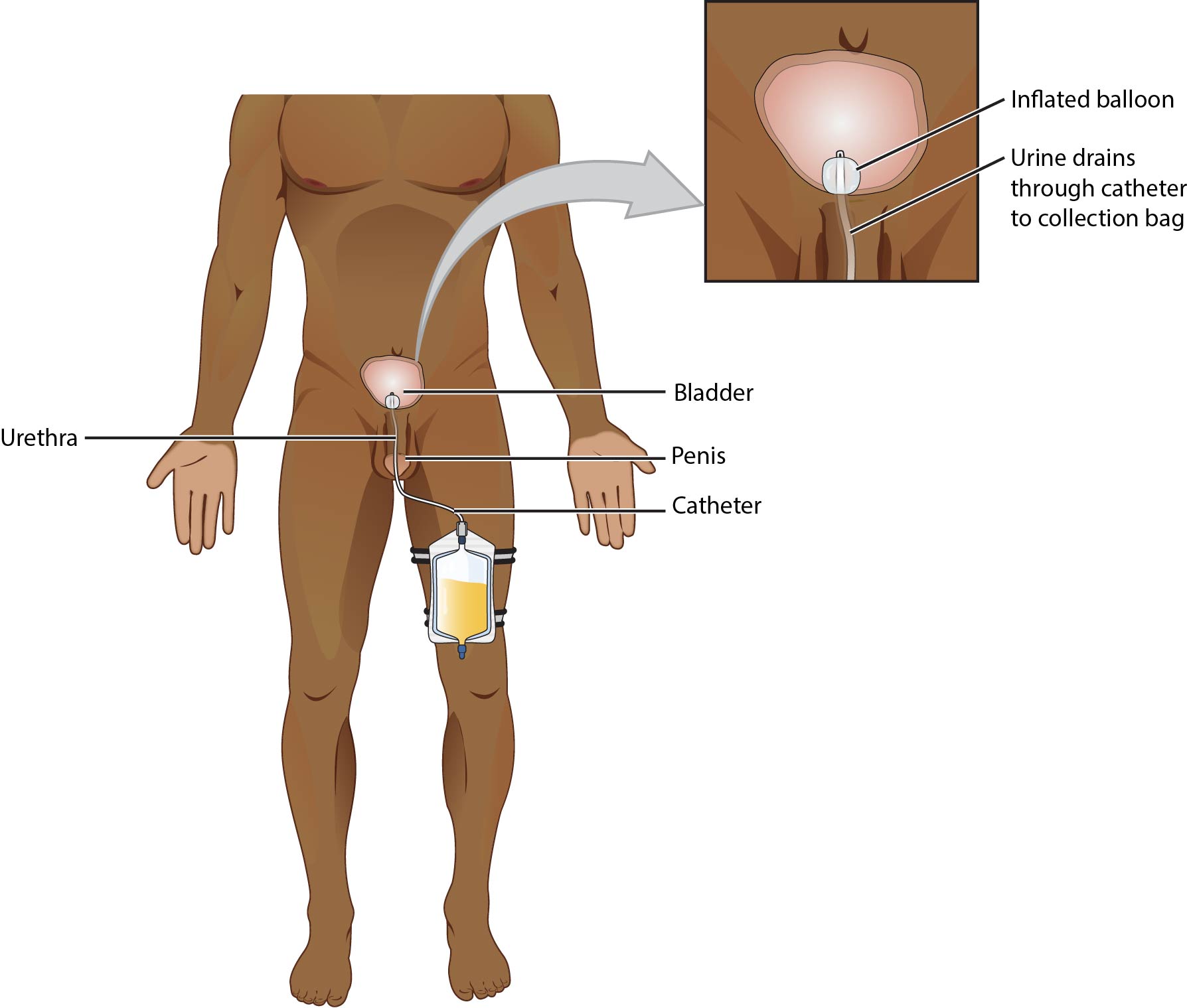 Illustration reference: OpenStax Clinical Nursing Skills Ch.19.4.
Illustration reference: OpenStax Clinical Nursing Skills Ch.19.4.
- Intermittent/straight catheter: Single-use in-and-out catheterization for retention relief or sterile specimen collection when clean void is not feasible.
- Device anatomy features: Drainage port for urine outflow and balloon-inflation port labeled with required inflation volume.
- French sizing scale: Larger French number indicates larger catheter diameter.
- Collection-bag options:
- larger bedside/inpatient bag (commonly up to about 2 L capacity)
- leg bag option for community mobility/discretion with more frequent emptying needs
- Coude tip catheter: Curved tip used especially for difficult male catheterization (for example enlarged prostate) with strict anterior orientation during insertion.
- Irrigation catheter: Larger lumen catheter (for example 20 Fr) used after selected prostate procedures for bladder irrigation and clot prevention/clearance.
- Suprapubic catheter: Surgically placed through abdominal wall into bladder when urethral pathway is unavailable or unsuitable.
- Male external (condom) catheter: Noninvasive penile external device connected to drainage bag for incontinence management and perineal-skin protection.
- Female external urinary catheter (FEUC): External wick device over meatus connected to low suction; preliminary evidence supports lower CAUTI exposure versus indwelling pathways in selected patients.
Nursing Assessment
NCLEX Focus
Prioritize dependent drainage safety and early contamination-risk detection every shift.
- Confirm catheter type and purpose (continuous drainage versus other elimination pathway).
- Before insertion, confirm need for positioning/visualization assistance (some settings require two-person insertion support).
- In retention pathways, assess whether intermittent catheterization is feasible/preferred over prolonged indwelling use.
- Assess tubing for kinks, compression, coiling, and inadequate slack.
- Verify drainage bag remains below bladder level and does not touch the floor.
- Assess for urethral traction risk when reservoir fills; monitor fill level and empty before excessive weight develops.
- Trend urine characteristics and volume pattern for early complication cues.
- For coude use, confirm insertion-orientation cue (line-up/anterior direction) before advancement.
- For suprapubic systems, assess insertion-site skin integrity and cleaning adherence.
- For external catheter pathways, assess skin fit/tolerance and leakage pattern, and verify suction/canister function for FEUC systems.
Nursing Interventions
- Keep closed urinary drainage pathway intact and dependent to gravity.
- During insertion, use strict aseptic setup, including hand hygiene before/after manipulation and sterile gloves/equipment.
- Perform perineal cleansing before insertion and continue routine meatal/perineal hygiene afterward.
- Inflate retention balloon only after correct placement per manufacturer guidance; do not preinflate balloon before insertion.
- Empty bedside bags before excess load develops (commonly around half to two-thirds full).
- Maintain tubing slack to prevent accidental pulling and urethral injury during movement.
- Position and secure drainage reservoir to reduce reflux and contamination risk.
- Use leg bags when mobility/discretion goals are prioritized, with higher-frequency emptying workflow.
- When clinically feasible, prioritize intermittent catheterization over indwelling pathways to reduce CAUTI exposure.
- Use coude catheters with correct anterior orientation to reduce urethral injury risk in difficult male catheterization.
- For suprapubic devices, perform regular insertion-site care per policy to prevent skin breakdown and local infection.
- For male incontinence management, consider condom-catheter pathway when clinically appropriate as a noninvasive alternative to indwelling catheterization.
- For eligible female patients, consider FEUC pathway with low-suction setup to limit indwelling-catheter days and reduce CAUTI risk.
- Reinforce CAUTI-prevention bundle behaviors: hand hygiene, closed-system protection, and daily necessity review.
Drainage-System Failure Risk
Bag elevation above bladder level, floor contact, or obstructed tubing can quickly increase reflux, trauma, and infection risk.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| diuretics | Furosemide, hydrochlorothiazide | Increased urine volume may require closer drainage-bag monitoring and earlier emptying. |
| antibiotics | Culture-guided UTI treatment | Do not substitute antibiotics for poor catheter-system technique; prioritize prevention workflow first. |
Clinical Judgment Application
Clinical Scenario
A postoperative patient with a Foley catheter reports urethral discomfort. The drainage bag is nearly full, tubing is partially kinked, and the bag is resting on the bed frame.
- Recognize Cues: Full reservoir, obstructed flow, and unsafe bag positioning.
- Analyze Cues: Current setup increases traction, stasis, and contamination risk.
- Prioritize Hypotheses: Immediate concern is preventable catheter-related harm and CAUTI risk escalation.
- Generate Solutions: Empty bag, unkink tubing, resecure reservoir below bladder, and reassess comfort/output.
- Take Action: Correct setup now and reinforce catheter-safety checks in ongoing care.
- Evaluate Outcomes: Flow normalizes, discomfort improves, and contamination risk decreases.
Related Concepts
- catheter-care-assistance - Daily urethral-to-tubing hygiene workflow.
- emptying-catheter-drainage-bag - Aseptic reservoir-emptying and output measurement sequence.
- cauti-prevention-and-catheter-necessity-review - Indication screening, daily necessity documentation, and catheter-day reduction framework.
- catheterization-nursing-process-and-troubleshooting - Pre-insertion nursing-process assessment and response to unexpected insertion findings.
- straight-catheterization-with-sterile-specimen-collection - Intermittent in-and-out catheterization steps for drainage and sterile specimen collection.
- bladder-assessment - Interpretation of urine-output and urinary-symptom cues.
- postvoid-residual-measurement-and-retention-management - Retention diagnostics and decompression escalation.
- urostomy-care-and-complication-surveillance - Urinary diversion stoma management, pouch routines, and complication surveillance.
- urinary-tract-infections - Device-related infection recognition and prevention priorities.