Caring for Clients with Developmental Disorders
Key Points
- Developmental disorders affect intellectual and adaptive functioning across daily life domains.
- Care planning should match support level to severity while maximizing independence and dignity.
- Consistent routines, clear communication, and safety-focused supervision improve quality of life.
Pathophysiology
Developmental disorders arise from brain or central nervous system impairment due to prenatal, perinatal, early-childhood, or genetic factors. Functional effects can include limits in problem-solving, communication, social interpretation, and self-management across settings.
Adaptive functioning determines day-to-day support needs more directly than diagnosis label alone. Severity ranges from mild to profound, requiring graduated assistance from cueing/supervision to full-time support.
Classification
- Mild impairment: Relative ADL independence with support for complex decisions (for example health, legal, and financial decisions) and higher-level life skills.
- Moderate impairment: Consistent verbal cueing/supervision for ADL completion, social interpretation, and major life decisions.
- Severe to profound impairment: Extensive to total support for communication, ADLs, safety, and continuous supervision.
- Condition-specific contexts: Down syndrome (Trisomy 21) and autism spectrum profiles with distinct support patterns.
- Condition-specific contexts: Down syndrome (Trisomy 21), autism spectrum profiles, cerebral palsy movement disorders, and intellectual-disability syndromes with distinct support patterns.
- Timing-of-injury contexts: Preconception/genetic, prenatal, perinatal, and early-childhood injury pathways that can shape lifelong neurodevelopmental outcomes.
- Intellectual-disability diagnostic context: Diagnosis combines intellectual-function testing with adaptive-function measurement rather than IQ alone.
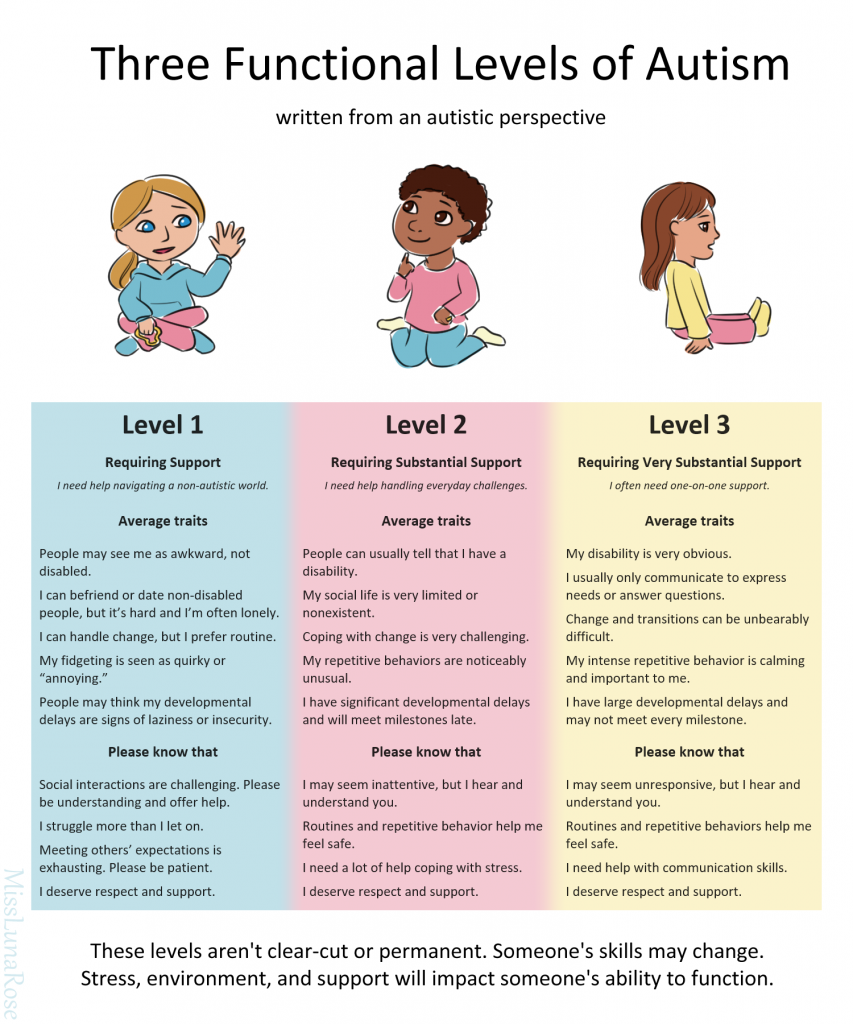 Illustration reference: OpenRN Nursing Assistant Ch.10.3.
Illustration reference: OpenRN Nursing Assistant Ch.10.3.
Nursing Assessment
NCLEX Focus
Priority questions focus on matching communication and supervision level to functional capacity rather than chronological age.
- Assess baseline communication method, comprehension level, and response to cues.
- Assess ADL independence, decision-making capacity, and supervision needs.
- Assess developmental-history timeline and prior screening findings (movement, language, behavior, cognition) and compare current function against age-expected milestones.
- In suspected intellectual impairment, assess for potentially confounding neurologic, visual, and hearing disorders before final classification.
- Identify sensory overload triggers, behavior escalation cues, and safety vulnerabilities.
- Screen for condition-specific clues when indicated: cerebral-palsy motor rigidity/ataxia/seizure or speech delay patterns, intellectual-disability learning/adaptive delays, and prenatal-injury signatures (for example fetal-alcohol-spectrum facial-growth/learning patterns).
- For infant cerebral-palsy screening contexts, monitor early red flags such as persistent head lag, very stiff or very floppy extremities, scissoring legs, delayed rolling beyond 6 months, and asymmetric or absent crawling pattern.
- For intellectual-disability diagnostic pathways, document standardized cognitive-testing context and adaptive-function burden in communication, social, and practical-skill domains.
- In prenatal-injury contexts, screen exposure/risk history for substance use, severe stress, environmental toxins (for example lead/mercury/pesticide exposure), unsafe pregnancy medications, malnutrition, or placental-insufficiency/IUGR patterns.
- Monitor for associated medical risks (for example, aspiration, injury, sleep concerns, or comorbidity trends), including Down syndrome-associated hearing loss, obstructive sleep apnea, congenital heart disease, and thyroid disorders.
- For Down syndrome care contexts, include surveillance for GI disorders (reflux/celiac patterns), hematologic abnormalities, and upper-cervical instability precautions relevant to activity and anesthesia planning.
Nursing Interventions
- Use simple, concrete, stepwise instructions and allow extra processing time.
- Maintain predictable routine and environment to reduce anxiety and disruptive behavior.
- Offer choices to support autonomy while preserving safety and task completion.
- Reapproach tasks calmly after de-escalation rather than forcing completion during distress.
- Use strengths-based encouragement and structured social participation to reinforce self-esteem and independence goals.
- Coordinate multidisciplinary referral pathways early (for example developmental specialists, therapy services, school-based supports, and family-resource navigation).
- In cerebral-palsy care contexts, reinforce symptom-focused plans (medication, bracing/adaptive devices, PT/OT, and selected surgical pathways for severe functional limitation).
Overstimulation and Safety Risk
Rapid environmental changes or sensory overload can trigger behaviors that increase injury risk for client and caregivers.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| psychotropic-medications (psychotropic-support-medications) | Condition-specific management context | Observe behavior/function changes and report adverse effects impacting ADLs or safety. |
| sleep-support-measures | Sleep-quality management context | Sleep disruption can worsen behavior regulation and adaptive functioning. |
Clinical Judgment Application
Clinical Scenario
A client with autism becomes increasingly agitated during morning care after unexpected staff and schedule changes.
- Recognize Cues: Escalating distress linked to routine disruption and sensory overload.
- Analyze Cues: Behavior reflects overwhelmed processing rather than intentional noncompliance.
- Prioritize Hypotheses: Immediate priority is safety and de-escalation.
- Generate Solutions: Reduce stimulation, use familiar cues, offer simple choices, and reapproach task later.
- Take Action: Implement calming routine and notify nurse of trigger pattern.
- Evaluate Outcomes: Client regains calm and care can proceed safely.
Related Concepts
- autism-spectrum-disorder - Communication/sensory differences require individualized care approach.
- congenital-genetic-and-acquired-complications - Common developmental-disorder profile with distinct health considerations.
- therapeutic-communication - Core skill for trust-building and behavior support.
- caring-for-clients-with-mental-health-or-substance-use-disorders - Shared principles in routine, empathy, and safety.
- fall-prevention - Functional and sensory factors increase injury risk.
Self-Check
- Why is adaptive functioning often a better care-planning guide than diagnosis label alone?
- Which communication strategy best supports safe ADL participation in moderate impairment?
- How should caregivers respond when behavior escalates during a nonurgent task?