Autism Spectrum Disorder
Key Points
- ASD is a neurodevelopmental condition characterized by social-communication differences and restricted/repetitive patterns.
- Symptom presentation and support needs vary widely, requiring individualized care planning.
- Early screening and diagnosis enable earlier intervention and better developmental outcomes.
- Effective care is interdisciplinary, family-centered, and strengths-based across home, school, and community.
- ASD occurs across racial/ethnic/economic groups; U.S. childhood prevalence is substantial (about 1 in 36), with higher diagnosed rates in males.
Pathophysiology
Autism Spectrum Disorder reflects neurodevelopmental differences in social communication, sensory processing, and behavioral regulation. Etiology is multifactorial and may include genetic risk, prenatal/perinatal factors, and developmental brain network variation.
Core features include differences in social reciprocity, communication style, and restricted/repetitive behaviors. Sensory sensitivity and emotional dysregulation can increase daily distress if environments are not adapted.
Many individuals with ASD also demonstrate strengths such as detailed long-term memory, strong visual/auditory learning, and high performance in selected domains (for example math, science, music, or art).
Recognized risk patterns include a sibling with ASD, older parental age at birth, specific genetic conditions (for example Down syndrome and Fragile X syndrome), and very low birth weight.
Classification
- Social-communication domain: Eye contact, conversational reciprocity, and social cue interpretation differences.
- Restricted/repetitive domain: Stereotypic motor patterns (for example hand flapping/rocking), compulsive arranging behaviors, resistance to change, restricted interests, and possible self-injurious patterns.
- Support levels: Level 1 (some support), Level 2 (substantial support), Level 3 (very substantial support).
- Intervention domains: Behavioral, developmental, educational, social-relational, pharmacologic, psychological, and complementary/alternative supports.
Nursing Assessment
NCLEX Focus
Identify functional support needs, sensory triggers, and family capacity rather than relying on labels alone.
-
Assess developmental history, communication profile, and social interaction patterns.
-
Reinforce routine developmental-milestone screening at well-child visits and autism-specific screening windows around 18 and 24 months.
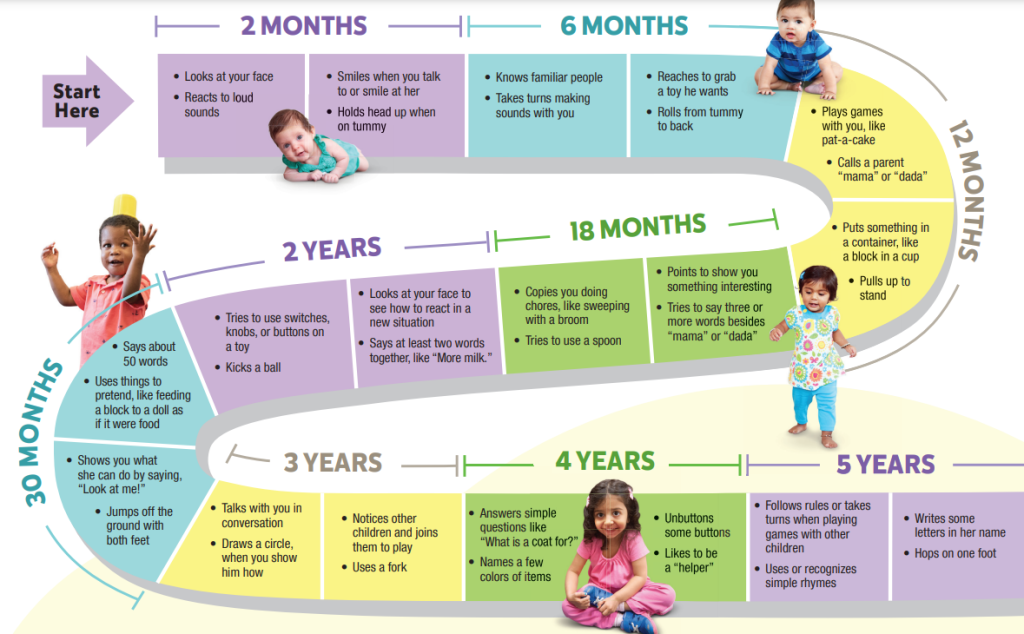 Illustration reference: OpenRN Nursing Health Promotion Ch.7.17.
Illustration reference: OpenRN Nursing Health Promotion Ch.7.17. -
Assess early social-communication cues (for example response to name, eye contact, and turn-taking) in developmental history.
-
When developmental delays are detected, support formal ASD screening workflows using caregiver report plus clinical observation tools and coordinate specialist developmental evaluation.
-
Use parent-completed autism tools (for example M-CHAT-R/F) as part of structured early-screen workflows.
-
Assess repetitive behaviors, sensory sensitivities, and emotional regulation triggers.
-
Assess common comorbidities (for example insomnia, ADHD, intellectual disability, anxiety, and depression) and their functional impact.
-
Assess safety risks, including elopement, self-injury, and vulnerability to abuse.
-
Assess caregiver-identified nonverbal pain and distress cues when the child cannot reliably self-report.
-
Assess family stressors, insurance/resource barriers, and sibling impact.
-
Assess current therapies and school supports, including IEP or communication devices.
Nursing Interventions
- Support early referral to developmental, speech, occupational, and behavioral services.
- Help families navigate special health-care and educational-needs pathways after diagnosis (for example chronic-condition management planning and service coordination).
- Collaborate with families to build structured routines and sensory-informed environments.
- Reinforce behavior plans that clarify antecedents and consequences to improve predictable learning and behavior shaping.
- Support applied behavior analysis (ABA) plans that promote desired behaviors, reduce harmful/disruptive behaviors, and track measurable progress over time.
- Use low-stimulation de-escalation strategies (for example dimmed lighting, noise reduction, and calming sensory supports) during agitation.
- Use clear, concrete communication and visual supports when indicated.
- For minimally verbal children, support alternative communication pathways (signs, picture systems, and electronic AAC devices).
- Support developmental therapies: speech-language, OT (including sensory integration), and PT to strengthen communication and adaptive function.
- Coordinate educational supports through IEP teams (parents/case worker/school staff) with visual schedules, structured classroom routines, and updated accommodations as needs change.
- Reinforce TEACCH-style classroom strategies (consistent routines, clear station boundaries, visual-first instruction, and paired verbal-plus-demonstration teaching) to improve learning participation.
- Encourage social-relational interventions (for example social stories and structured social-skills groups) to practice interaction in predictable settings.
- Coordinate referral for adapted CBT when anxiety, depression, or rigid stress responses interfere with daily function.
- Promote strengths-based goals in education, social engagement, and daily living skills.
- Coordinate interdisciplinary follow-up across developmental stages and transitions.
- As adolescents with ASD move to adulthood, help coordinate transition supports for vocational training, employment access, housing, transportation, and community participation.
- Provide clear vaccine counseling that MMR does not cause autism and address misinformation using evidence-based teaching.
- Anticipate caregiver role strain and teach practical stress-management strategies (exercise, healthy nutrition, boundaries, social supports, grounding, mindfulness, breathing, values-based coping).
- Refer families to ASD-focused support organizations and community resources (for example Autism Society, Autism Speaks, and state-based parent information/resource centers).
One-Size-Fits-All Harm
Standardized approaches without individual adaptation can increase distress and reduce participation.
Pharmacology
No medication cures ASD. Pharmacologic care is symptom-targeted for associated concerns such as high activity, inattention, irritability/aggression, self-injurious behavior, sleep disturbance, anxiety/depression, or seizure comorbidity in collaboration with prescribers.
Nurses monitor efficacy, adverse effects, and function while reinforcing behavioral and developmental interventions as core treatment.
Some families use complementary approaches (for example special diets, herbal products, animal-assisted activities, art therapy, mindfulness, or relaxation). Nurses should review safety, interaction risk, and goal alignment while reinforcing that adjunctive approaches do not replace core evidence-based supports.
Clinical Judgment Application
Clinical Scenario
A preschool child has delayed social reciprocity, frequent hand-flapping, intense distress with routine changes, and limited expressive language.
- Recognize Cues: Multi-domain ASD features with sensory-triggered dysregulation.
- Analyze Cues: Pattern supports ASD with substantial support needs.
- Prioritize Hypotheses: Priorities are communication support, safety, and family coaching.
- Generate Solutions: Build an interdisciplinary plan with school and therapy integration.
- Take Action: Implement visual routine supports and caregiver education.
- Evaluate Outcomes: Reduced dysregulation and improved daily participation.
Related Concepts
- communication-disorders - Language/pragmatic challenges frequently overlap.
- intellectual-disabilities - May coexist and influence adaptive planning.
- attention-deficit-hyperactivity-disorder - Shared attention and regulation concerns are common.
- anxiety-related-disorders - Anxiety can increase rigidity and sensory distress.
- family-support-systems - Family adaptation is central to long-term outcomes.