Therapeutic Exercise Types for Functional Ability
Key Points
- Therapeutic exercise uses intentional movement to restore strength, endurance, ROM, and flexibility for daily function.
- ROM and stretching improve joint mobility and reduce muscle tension when performed with proper form.
- Balance exercise lowers fall risk by training body alignment and control.
- Isometric and isotonic exercises build strength through different muscle-loading patterns.
- Isokinetic exercise keeps movement speed constant while resistance varies, often in rehabilitation settings.
- Aerobic exercise increases heart and respiratory rate and supports endurance for sustained ADL performance.
- Combined strength, aerobic, balance, and mobility work supports fall-risk reduction, ADL performance, sleep, and psychosocial well-being.
Pathophysiology
Functional decline often follows reduced activity, pain, or prolonged illness. Targeted exercise improves neuromuscular recruitment, joint mobility, and movement confidence, which supports safer performance of ADLs.
Regular activity can also support broader health goals, including mood improvement, chronic-disease risk reduction, bone-health maintenance in older adults, and reduced social isolation when performed in groups.
Most therapeutic movements are interpreted by how joint angles change (for example flexion vs extension) or how a limb moves relative to the body’s midline (abduction vs adduction). Planning exercise with these paired movement patterns helps nurses cue safer, more intentional repetitions. Resistance-focused training can improve muscle strength/endurance, cartilage and bone health, posture, and functional capacity, and may also support pain reduction, sleep quality, and cardiometabolic risk reduction.
Poor technique or abrupt intensity increases can cause strain and injury. Safe benefit depends on gradual progression and movement quality.
Classification
- ROM and stretching exercise: Joint-focused movements (for example hip, knee, shoulder, elbow flexion/extension) plus muscle-lengthening work to improve mobility and reduce tension.
- Movement-direction framework: Flexion/extension, abduction/adduction, and circumduction or rotation patterns are paired intentionally to train controlled movement through full range.
- Balance exercise: Control and alignment drills such as supported single-leg stance, high-knee marching, and heel raises.
- Targets static and dynamic postural control, reaction time, and center-of-gravity management to reduce fall risk.
- Isometric exercise: Muscle contraction with minimal joint movement, often held about 5-10 seconds before release; useful for stabilization and foundational strength.
- Isotonic exercise: Resistance through a movement range with both concentric and eccentric contraction phases; examples include pushups, squats, bicep curls, and lunges.
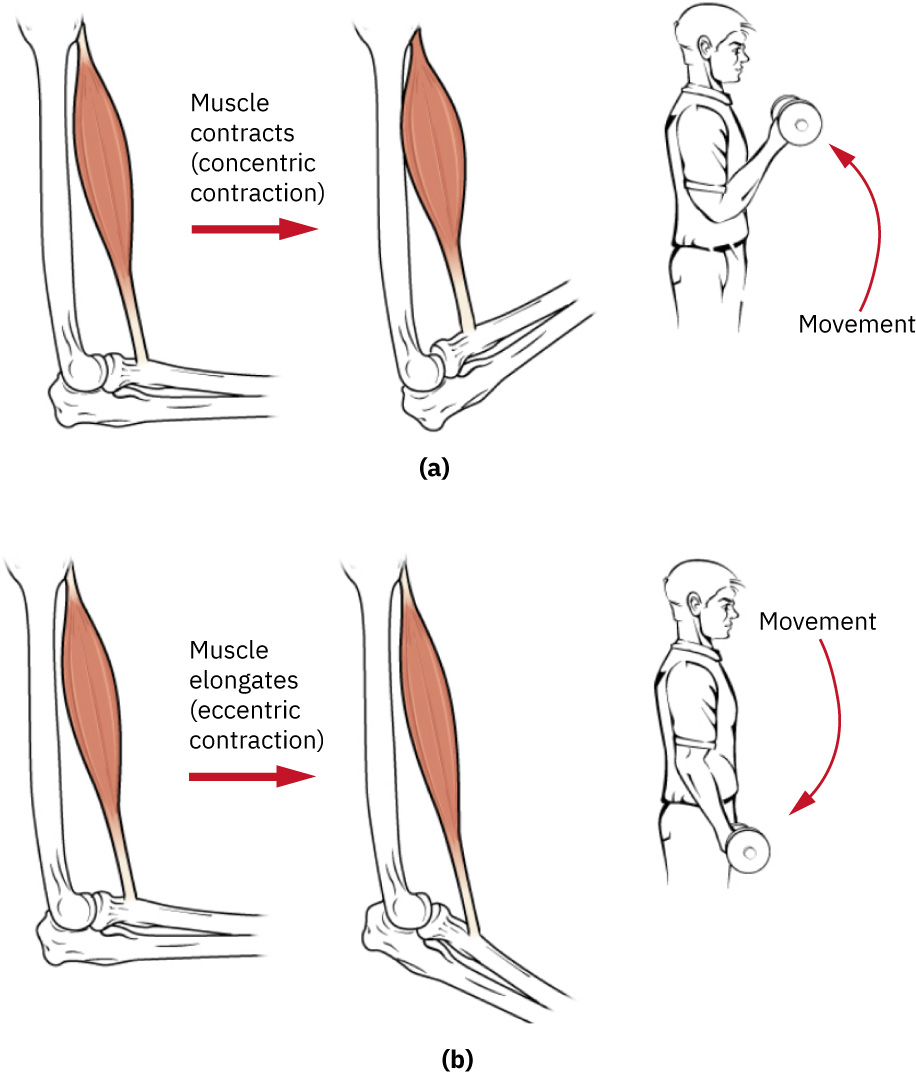 Illustration reference: OpenStax Clinical Nursing Skills Ch.9.
Illustration reference: OpenStax Clinical Nursing Skills Ch.9. - Isokinetic exercise: Constant-speed movement with variable resistance; frequently therapist-guided and equipment-assisted, though resistance-band workflows can support similar training goals.
- Aerobic exercise: Cardiovascular activity that raises heart and breathing rate (for example walking, stair climbing, low-intensity marching-in-place, or sit-to-stand intervals).
- Effective aerobic benefit requires sustained bouts of at least several minutes and enough cumulative active time across the day.
- Expected adaptations include improved oxygen use, higher stroke volume, and lower resting heart-rate burden over time.
Nursing Assessment
NCLEX Focus
Questions commonly test exercise-type differentiation and selection for a specific functional deficit.
- Assess baseline mobility, pain, strength, and tolerance before initiating exercise.
- Assess baseline physical-activity pattern across work, home, transportation, and leisure domains to avoid underestimating true activity load.
- Assess social and access barriers to activity (for example cost, transportation, childcare/time constraints, and housing insecurity).
- Assess baseline cardiopulmonary tolerance and exertional symptoms before aerobic progression.
- Assess movement quality and form during exercise, not only task completion.
- Assess whether exercise selection matches the target ADL problem (for example sit-to-stand weakness).
- Reassess fatigue, pain response, and fall risk as intensity progresses.
Nursing Interventions
- Coordinate exercise planning with PT/OT and align goals to current ADL barriers.
- Start at tolerated intensity and progress gradually to reduce injury risk.
- Keep stretching slow and steady; stop short of pain and avoid forceful end-range pushing.
- Use warm-up and cooldown periods for aerobic sessions to reduce injury risk and support safe recovery to baseline.
- For isokinetic-focused plans, confirm device setup and therapist parameters before unsupervised repetitions.
- Provide clear step-by-step cueing for posture, tempo, and breathing.
- Pair exercise selection with ADL goals:
- for sit-to-stand difficulty, use controlled bodyweight squat progressions
- for poor joint mobility, prioritize ROM/stretching sequence
- for instability, add supervised balance drills with support
- For aerobic conditioning, begin with low-intensity intervals and increase duration toward sustained activity targets as tolerated.
- Use brief activity bouts across the day when fatigue, schedule pressure, or low confidence makes longer sessions unrealistic.
- On high-stress days, lower exercise intensity instead of stopping all movement to prevent sedentary backslide.
- Teach that effective activity plans can remain simple and safe (for example chair-based ROM/isometric/isotonic drills plus community walking).
- When access barriers exist, prioritize feasible low-cost options (for example walking groups, home-based routines, and community resource linkage).
- Coordinate interprofessional planning with nursing, PT, and OT so exercise prescriptions match medical status and functional goals.
- Stop and reassess if pain sharply worsens, form breaks down, or dizziness develops.
Technique Safety Priority
Incorrect form during strengthening or stretching can worsen pain and increase injury risk.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| analgesics | Activity-limited pain contexts | Time exercise after pain control to improve participation and movement quality. |
| sedatives | Sleep/anxiety medications | Sedation can impair form, reaction time, and balance; increase supervision level. |
Clinical Judgment Application
Clinical Scenario
A patient recovering from hospitalization struggles to rise from a chair and demonstrates low confidence with standing.
- Recognize Cues: Sit-to-stand weakness and reduced movement confidence.
- Analyze Cues: Lower-body strength and balance deficits are limiting ADL independence.
- Prioritize Hypotheses: Priority is safe functional-strength recovery without falls.
- Generate Solutions: Add supervised slow squat progression, balance drills, and ROM warm-up.
- Take Action: Implement short, frequent sessions with technique cueing and rest intervals.
- Evaluate Outcomes: Sit-to-stand performance and ADL independence improve without injury.
Related Concepts
- promoting-joint-mobility-and-activity - Daily mobility plan that embeds functional exercise into care.
- assisting-with-ambulation - Walking support should reflect current strength and balance tolerance.
- fall-prevention - Balance and mobility training reduce fall risk when paired with environmental controls.
- activities-of-daily-living - Exercise selection should map to specific ADL limitations.
Self-Check
- How do isometric and isotonic exercises differ in movement and loading?
- Why should nurses map exercise type to a specific ADL deficit?
- Which findings indicate exercise intensity should be reduced or paused?