Bipolar Disorders
Key Points
- Bipolar disorders involve recurrent mood polarity shifts between depression and mania/hypomania.
- Mania requires at least one week of persistently elevated or irritable mood with increased energy and marked functional impairment; severe episodes may require hospitalization and can progress to psychosis.
- A single confirmed manic episode can shift diagnosis from unipolar depression to bipolar-spectrum illness.
- Bipolar I includes mania plus depression; Bipolar II includes hypomania plus depression; cyclothymia includes subthreshold fluctuating symptoms.
Other specifiedandunspecifiedbipolar diagnoses are used when bipolar-like symptoms are clinically significant but do not fully meet Bipolar I/II/cyclothymia criteria.- Severe manic psychosis can resemble schizophrenia-spectrum presentations; differential diagnosis depends on longitudinal mood-episode pattern, not one cross-sectional psychotic snapshot alone.
- Acute manic phases require safety, structure, and clear communication boundaries.
- Bipolar depressive phases carry major suicide risk; suicide mortality is reported around 20 times higher than the general population in some cohorts.
- Long-term outcomes improve with combined medication, psychotherapy, rhythm/relapse management, and escalation to ECT or other brain-stimulation options when severe symptoms persist despite standard treatment.
- Nursing care adapts across phases while preserving autonomy, dignity, and continuity.
Pathophysiology
Bipolar disorders likely arise from interacting genetic vulnerability, neurotransmitter dysregulation, circadian instability, and environmental stress triggers. Polarity shifts alter sleep, judgment, impulse control, and functional capacity.
Comorbid anxiety, substance use, and suicidality increase complexity and risk.
Emerging neurobiologic work also suggests altered intracellular calcium signaling in bipolar-spectrum illness, which aligns with observed benefit of selected antiseizure mood-stabilizing agents in some treatment plans.
Depressive episodes with mixed features are an important risk signal because they can precede later Bipolar I/II diagnostic evolution in some clients.
Classification
- Polarity states: Depressive episodes, manic episodes, hypomanic episodes, and mixed features.
- Bipolar I disorder: Manic episode (with or without psychosis) plus depressive episodes over time.
- Bipolar II disorder: Hypomanic episodes and depressive episodes without full mania.
- Cyclothymia: Mood fluctuations with hypomanic/depressive symptoms that do not meet full bipolar criteria.
- Other specified/unspecified bipolar disorders: Bipolar-pattern symptoms with clinically relevant distress/impairment that do not fit full criteria for the core bipolar categories.
- Rapid-cycling pattern: At least 4 manic/hypomanic/depressive episodes within 12 months; may present with very short cycle intervals and higher functional burden.
- Severity context: Symptom burden ranges from mild functional disruption to hospitalization-level crises.
- Treatment phase: Acute stabilization versus maintenance/relapse prevention.
Episode Criteria Snapshot
- Manic episode: Elevated/irritable mood plus increased energy for at least 1 week with marked functional impairment; hospitalization may be required.
- Hypomanic episode: Similar symptom cluster for at least 4 consecutive days with observable change, but no marked impairment/hospitalization.
- Psychosis rule: If psychotic features are present, the episode is classified as mania by definition.
- Bipolar depressive episode: At least 2 weeks with at least 5 depressive symptoms, including depressed mood or loss of interest/pleasure.
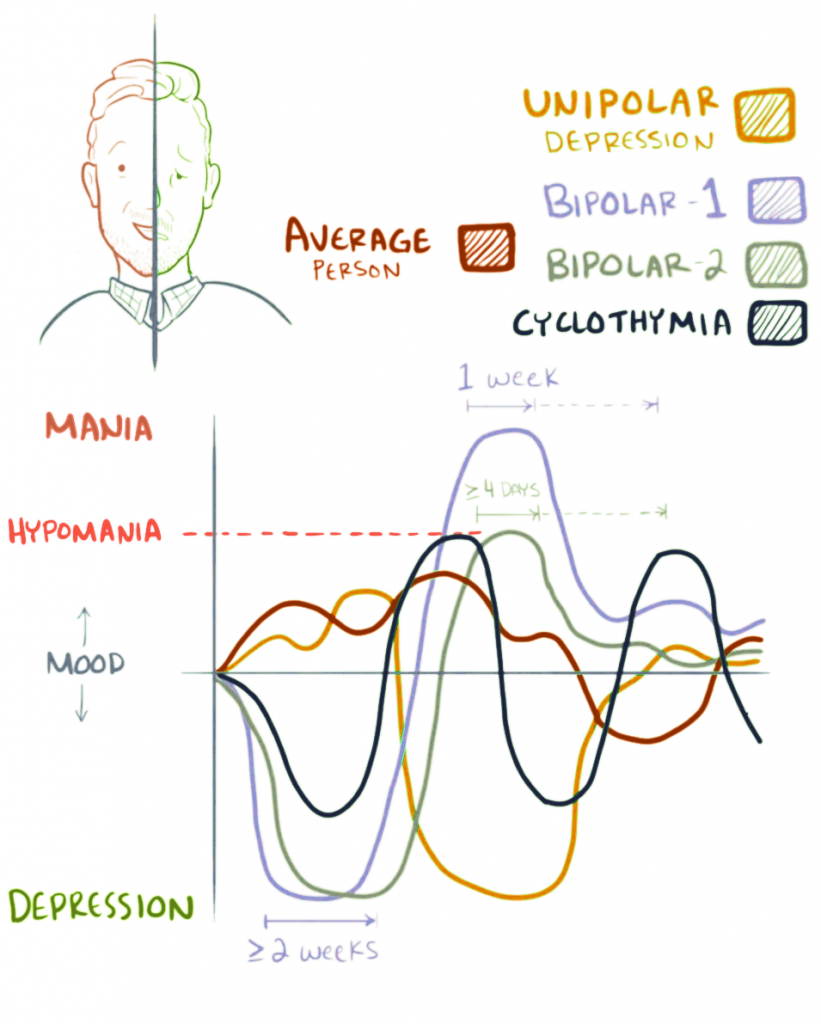 Illustration reference: OpenRN Nursing Mental Health and Community Concepts 2e Ch.8.2.
Illustration reference: OpenRN Nursing Mental Health and Community Concepts 2e Ch.8.2.
Nursing Assessment
NCLEX Focus
Differentiate mania from hypomania and assess immediate safety/impulsivity risk first.
- Assess current polarity state, symptom intensity, and psychosis presence.
- When mania, hypomania, or psychosis reduces insight, obtain collateral history from family/significant others to improve chronology and risk accuracy.
- Assess classic manic cues: grandiosity, decreased need for sleep, pressured speech, flight of ideas/racing thoughts, distractibility, goal-directed overactivity, and high-risk behaviors.
- During manic MSE, document orientation variability, labile euphoric-to-irritable mood, provocative/flamboyant or neglected grooming, hyperverbal/pressured speech, loose/clang associations, hallucination/paranoia cues, and impaired attention/judgment.
- When psychosis is present, assess longitudinal mood chronology and prior episode pattern to distinguish bipolar-spectrum psychosis from primary psychotic-disorder trajectories.
- Assess sleep disruption, impulsivity, risk-taking behavior, and suicidal ideation.
- Assess self-harm and other-directed danger together (suicidal, homicidal, or violence ideation), including impulse-linked legal/financial harms (for example reckless spending) that may require temporary external controls.
- During bipolar depressive phases, assess for psychotic depressive content (for example guilt/catastrophe delusions or voices reinforcing worthlessness) with immediate suicide-risk escalation when present.
- Assess coexisting disorders (for example anxiety disorders, ADHD, substance-use disorders, and eating-disorder patterns) because comorbidity changes risk and treatment prioritization.
- On initial manic evaluation, screen for thyroid dysfunction and substance intoxication/withdrawal patterns (for example alcohol, sedatives, cocaine, methamphetamine, PCP) that can mimic bipolar-spectrum episodes.
- Use bipolar-focused tools for baseline and trend tracking when available (for example MDQ, YMRS including parent versions, and Altman Self-Rating Mania Scale).
- Assess physiologic instability during mania, including dehydration risk, poor nutrition/fluid intake, sleep loss, constipation, hygiene deficits, and electrolyte abnormalities.
- Include baseline medical workup for suspected bipolar episodes (TSH, CBC, chemistry panel, urine toxicology) and trend medication-safety labs (therapeutic drug levels, kidney/liver function, thyroid/calcium, sodium, hematocrit, albumin, prealbumin) as treatment evolves.
- Begin psychosocial assessment with the client’s own words, then use focused prompts (for example PQRSTU) to clarify manic-trigger patterns, symptom intensity, duration, and insight.
- Integrate cultural-formulation and spiritual-history questions (for example CFI/FICA domains) to individualize care and avoid mislabeling culturally normative or spiritually framed experiences.
- Assess medication adherence, side effects, and prior response history.
- Assess co-occurring substance use and social determinant stressors.
- In pediatric cases, assess overlap with ADHD/ODD/conduct/anxiety presentations and evaluate caregiver strain.
- In pediatric bipolar presentations, watch for prominent irritability, severe mood lability, sleep-pattern change, destructive outbursts, and depressive withdrawal/somatic complaints.
- In older adults, treat new-onset mania after about age 60 as atypical and escalate medical-cause evaluation (for example stroke, thyroid dysfunction, dementia).
- Assess family-dynamics quality (supportive versus conflictual/stress-amplifying) because it can change relapse risk and treatment adherence.
- Assess early relapse cues reported by client/family/supports.
Nursing Interventions
- In mania, use low-stimulation setting, concise directions, and firm respectful boundaries.
- During escalating mania, use short concrete statements, neutral limit-setting, and redirection; avoid power struggles, jokes/cliches, and exploratory probing.
- In depression, use empathic communication and active suicide-risk monitoring.
- During manic communication, maintain calm tone and clear directives while avoiding direct confrontation of grandiose content unless immediate safety requires redirection.
- Implement physiologic care during acute mania: frequent high-calorie/high-protein snacks and fluids (including finger foods), protected rest routines, caffeine avoidance, constipation prevention, and step-by-step hygiene cueing.
- During acute manic admission planning, target symptom stabilization plus safety with reduced stimulation/activity and protected sleep windows (often at least about 4-6 hours/night early in stabilization), while maintaining hydration and nutritional intake.
- Build bipolar care plans with common high-priority nursing diagnoses as indicated:
Risk for Injury,Risk for Suicide,Risk for Violence, impaired communication/cognition, self-care deficit, impaired nutrition, disturbed sleep, fatigue, social isolation, and risk for spiritual distress. - Separate outcome targets by illness phase: acute-mania goals emphasize immediate safety and physiologic stabilization; maintenance goals emphasize trigger prevention, therapy participation, and durable coping skills.
- Write phase-matched SMART outcomes (for example, communicate self-harm thoughts before acting during this shift; eat within one hour of meal delivery; attend scheduled outpatient group sessions daily during maintenance planning windows).
- Support medication adherence and routine lab/side-effect surveillance (for example lithium safety monitoring).
- Use APNA implementation domains to structure bipolar interventions: coordination of care, health teaching/health promotion, pharmacologic-biologic-integrative therapies, milieu therapy, and therapeutic relationship/counseling.
- In coordination-of-care work, keep interprofessional safety expectations consistent across staff, support transitions (admission/discharge), and connect clients to outpatient/community/peer-support or housing resources when indicated.
- In health-teaching work, reinforce early-warning-sign recognition, mood tracking, relapse-prevention routines, and substance-avoidance; address stigma and self-advocacy barriers.
- In pharmacologic/integrative work, teach expected medication-response timelines and toxicity cues, review monitoring labs, and use observed-medication administration safeguards when risk indicates (for example opening medications in front of the client).
- In milieu planning, maintain structured low-stimulation settings, avoid competitive activities during manic escalation, and secure valuables when judgment is unsafe to reduce financial or legal harm.
- During severe mania, prefer short 1:1 structured contacts over large-group programming until attention and boundaries improve.
- In maintenance-phase planning, assess and address post-episode consequences (interpersonal, occupational, educational, financial), treatment ambivalence, and substance self-medication patterns that increase relapse risk.
- For escalating agitation, attempt de-escalation early; if imminent injury risk persists, implement least-restrictive emergency containment and prescribed rapid-calming medication protocols per policy (for example antipsychotic +/- benzodiazepine).
- Teach bipolar self-management mainly when acute manic symptoms begin to settle because severe mania can reduce readiness for learning.
- Include practical education targets: treatment commitment, appointment adherence, medication adherence, daily structure (sleep/meals/activity), early warning signs (for example decreased need for sleep), stress-management skills, and support-group linkage.
- Reevaluate continuously against SMART goals: medical stability (nutrition/sleep/labs/activity), self-care engagement, self/other safety, therapeutic-milieu participation, boundary control, communication appropriateness, illness insight, medication tolerability at therapeutic levels, and discharge-plan participation.
- Use concise behavior-based documentation (for example SOAP-style) during acute mania with direct quotes for subjective statements and objective cues such as pressured speech, distractibility, intrusive behavior, activity excess, boundary violations, and current self/other-harm risk status.
- Reinforce maintenance tools such as self-care journaling (life charts) to track mood, sleep, treatments, and triggers over time.
- Reinforce psychoeducation on triggers, sleep regularity, and relapse-action plans.
- Integrate bipolar-focused psychotherapy pathways when available, including interpersonal and social rhythm therapy (IPSRT) and family-focused therapy.
- Coach lifestyle protection routines that support relapse prevention: regular aerobic activity (plus tolerated strength/flexibility work), consistent sleep-wake schedule, balanced dietary pattern, mindfulness/stress-regulation practice, and avoidance of alcohol/tobacco/recreational drugs.
- Coordinate psychotherapy and family-focused interventions to improve long-term stability.
Polarity Mismatch Treatment
Inadequate polarity assessment can lead to interventions that worsen instability (for example poorly monitored antidepressant activation).
Pharmacology
Core medication groups include mood stabilizers, selected atypical antipsychotics, and adjunctive therapies. Lithium can reduce manic symptoms within about 1-3 weeks, carries antisuicidal benefit, and requires strict blood-level monitoring (typical therapeutic ranges: about 0.8-1.2 mEq/L for acute goals and 0.8-1.0 mEq/L for maintenance goals; severe toxicity risk rises around or above 2.0 mEq/L). Valproate may reduce episode frequency/severity in selected clients. Nursing priorities include toxicity monitoring (notably lithium), interaction checks, hydration guidance, and adherence support through phase transitions.
In bipolar depressive episodes, antidepressants are generally used with a mood stabilizer and/or antipsychotic rather than as monotherapy because unopposed antidepressant exposure can precipitate manic switching.
Lithium teaching should include sodium and hydration balance (dehydration or sudden sodium shifts can precipitate toxicity) and stage-based toxicity cues: early GI upset/fine tremor/polyuria-weakness, moderate coarse tremor-confusion-unsteady gait, and severe seizures-coma-oliguria/anuria-arrhythmia requiring emergency escalation.
Clinical Judgment Application
Clinical Scenario
A client in acute mania has minimal sleep, pressured speech, grandiosity, spending sprees, and escalating irritability with refusal of routine medication.
- Recognize Cues: High-risk manic syndrome with impaired judgment and potential safety threats.
- Analyze Cues: Immediate stabilization is required before deeper insight-based interventions.
- Prioritize Hypotheses: Priority is behavioral safety and rapid mood stabilization.
- Generate Solutions: Implement structured milieu, medication support, and close monitoring.
- Take Action: Apply de-escalation, coordinate prescriber adjustments, and engage supports.
- Evaluate Outcomes: Track sleep restoration, agitation reduction, and improved decision control.
Related Concepts
- depressive-disorders - Covers depressive-polarity overlap and differential needs.
- the-spectrum-of-mood-disorders - Places bipolar illness within dimensional mood frameworks.
- self-harm-and-suicide - Addresses elevated suicidality risk across bipolar phases.
- psychopharmacology - Expands medication-mechanism and safety management details.
- client-engagement - Supports sustained adherence and relapse-prevention collaboration.