Chain of Infection
Key Points
- Infection spread follows six linked steps: agent, reservoir, portal of exit, mode of transmission, portal of entry, and susceptible host.
- Breaking any one link stops ongoing transmission.
- Transmission can occur directly between hosts or through one or more intermediate hosts.
- Causative agents include bacteria, viruses, fungi, and other pathogens that require specific growth conditions.
- The epidemiologic triad (host-agent-environment) complements the chain model by describing who is at risk, what pathogen is involved, and where transmission is enabled.
- Contact, droplet, and airborne spread are key transmission modes tested on NCLEX.
- Respiratory secretions and contaminated hands are common transmission vehicles; a single sneeze can release large pathogen loads into the environment.
- Asymptomatic carriers can still spread organisms such as mrsa or respiratory viruses.
- Reservoirs can be human, animal (zoonotic), or environmental, and each requires different control strategy.
- Routine hygiene and isolation precautions are core nursing strategies to interrupt transmission.
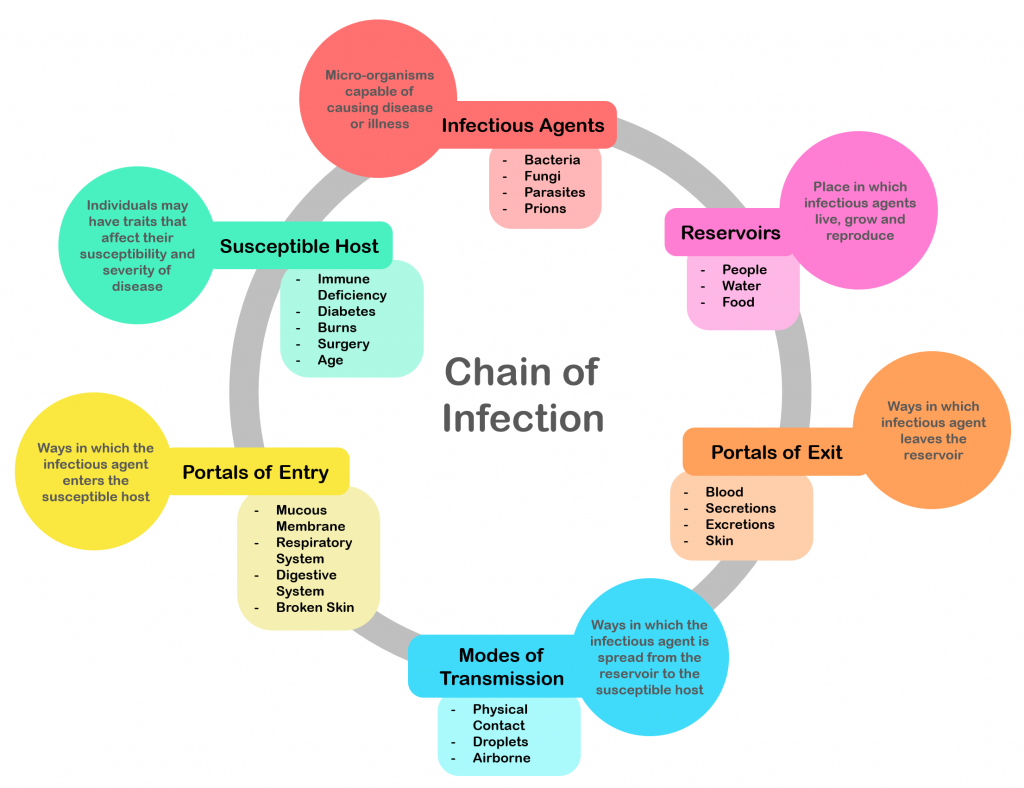 Illustration reference: OpenRN Nursing Fundamentals 2e Ch.9.6.
Illustration reference: OpenRN Nursing Fundamentals 2e Ch.9.6.
Pathophysiology
The chain of infection explains how a pathogen moves from reservoir to new host. The six links are infectious-agent, reservoir, portal-of-exit, mode-of-transmission, portal-of-entry, and susceptible-host. Infection occurs when all links remain intact long enough for organism transfer and host invasion.
The epidemiologic triad (host, agent, environment) provides an additional transmission framework that aligns with the six-link chain and helps organize prevention planning in bedside and public-health contexts.
Transmission may occur directly from one host to another or through a more complex pathway with intermediate hosts. This is why link-by-link interruption is required even when the immediate source is not obvious at bedside.
The model is clinically useful because it is actionable. If the nurse interrupts even one step, transmission fails. In practice, nurses most often break links through hand-hygiene, environmental cleaning, source control, and barrier precautions.
Causative agents span bacteria, viruses, fungi, protozoa, helminths, and prions. Pathogen growth depends on environmental fit (for example moisture, temperature, pH, oxygen availability, and water access). Agent behavior also reflects infectivity, ability to invade host tissue, toxin-production capacity, and overall virulence (disease severity).
Normal flora are usually protective, but flora behavior affects transmission risk. Resident flora persist in deeper skin layers and are not fully removed by routine hygiene, while transient flora acquired by contact are more effectively removed with handwashing.
Carriers may be asymptomatic but still transmit infection. The text describes colonization and carrier status, including healthcare workers carrying mrsa in the nares without active illness.
Some infectious diseases are communicable (contagious person-to-person spread), while others are infectious but primarily transmitted through nonhuman environmental pathways (for example water, food, soil, vectors, or animal-to-human routes).
If host response becomes dysregulated after infection is established, progression to severe systemic illness such as sepsis can occur.
Classification
- Contact transmission: Organism spread through direct touch or contaminated surfaces.
- Droplet transmission: Larger respiratory particles from cough or sneeze spread over short range.
- Airborne transmission: Smaller particles remain suspended and spread through air movement.
- Indirect transmission subtype: Vehicle-borne (food/water/fomites) and vector-borne (for example mosquito/tick) routes.
- Reservoir subtype: Human, animal, and environmental sources (soil/water/plants).
Nursing Assessment
NCLEX Focus
Questions often ask which transmission link is active and which nursing action breaks that link first.
- Identify likely Chain Of Infection and current reservoir.
- Determine actual or potential portal-of-exit (respiratory secretions, drainage, blood).
- Assess likely mode-of-transmission in the care setting.
- Evaluate patient factors that increase susceptible-host risk, including age extremes and chronic illness.
- Check for invasive devices that create an artificial portal-of-entry.
Nursing Interventions
- Perform strict hand-hygiene before and after every patient contact.
- Apply standard-precautions consistently for all patients.
- Escalate to transmission-based-precautions when organism route is known or suspected.
- Use appropriate personal-protective-equipment and correct donning/doffing sequence.
- Limit organism spread by cleaning shared equipment and high-touch surfaces.
- Follow proper contaminated-waste handling and disposal steps to reduce environmental reservoir burden.
- Teach patients and families respiratory etiquette and symptom reporting.
- Promote prevention behaviors that reduce host susceptibility, including vaccination, rest, nutrition, exercise, and stress management support.
Hand Hygiene Breakdowns
Missed hand hygiene can preserve all transmission links and lead to preventable spread between vulnerable patients.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Not specified in source | None provided in this section | Prioritize nonpharmacologic infection-prevention actions that break transmission links |
Clinical Judgment Application
Clinical Scenario
A nursing assistant helps a resident with a draining wound, then enters another room without hand hygiene. The second resident has diabetes and a urinary catheter.
- Recognize Cues: Drainage exposure, missed hand hygiene, indwelling catheter, chronic disease.
- Analyze Cues: Contact transmission risk is high and a portal of entry already exists.
- Prioritize Hypotheses: Imminent cross-transmission to a susceptible host.
- Generate Solutions: Immediate hand hygiene, glove change, equipment disinfection, and precaution reinforcement.
- Take Action: Stop care sequence, perform hand hygiene, apply correct PPE, and notify nurse.
- Evaluate Outcomes: No new infection signs, improved compliance with infection-control workflow.
Related Concepts
- standard-precautions - Universal baseline actions that interrupt multiple transmission links.
- transmission-based-precautions - Added measures for contact, droplet, or airborne spread.
- hand-hygiene - Highest-yield action for preventing cross-transmission.
- multidrug-resistant-organisms - Common healthcare organism with asymptomatic carrier potential.
- healthcare-associated-infections - Outcome when transmission is not interrupted in care settings.
- susceptible-host - Final link that determines clinical infection risk.
Self-Check
- Which single link can be interrupted most consistently by frontline nursing staff?
- How does an invasive device change portal-of-entry risk?
- Why can asymptomatic carriers still sustain transmission in healthcare units?