Irritable Bowel Syndrome
Key Points
- IBS is a chronic functional GI disorder: symptoms are present without a structural GI disease explaining them.
- IBS affects about 10% to 15% of people in the United States and is a frequent outpatient GI diagnosis.
- Core presentation is recurrent abdominal discomfort/pain with altered bowel pattern (constipation, diarrhea, or mixed pattern).
- Rome IV clinical criteria guide diagnosis; there is no single confirmatory diagnostic test.
- Management is individualized with lifestyle trigger control, stress reduction, and symptom-pattern-based pharmacology.
Pathophysiology
IBS is thought to involve dysregulated bowel motility and gut-brain signaling. Increased intestinal contractions can drive diarrhea-predominant symptoms, while reduced or weak contractions can drive constipation-predominant symptoms.
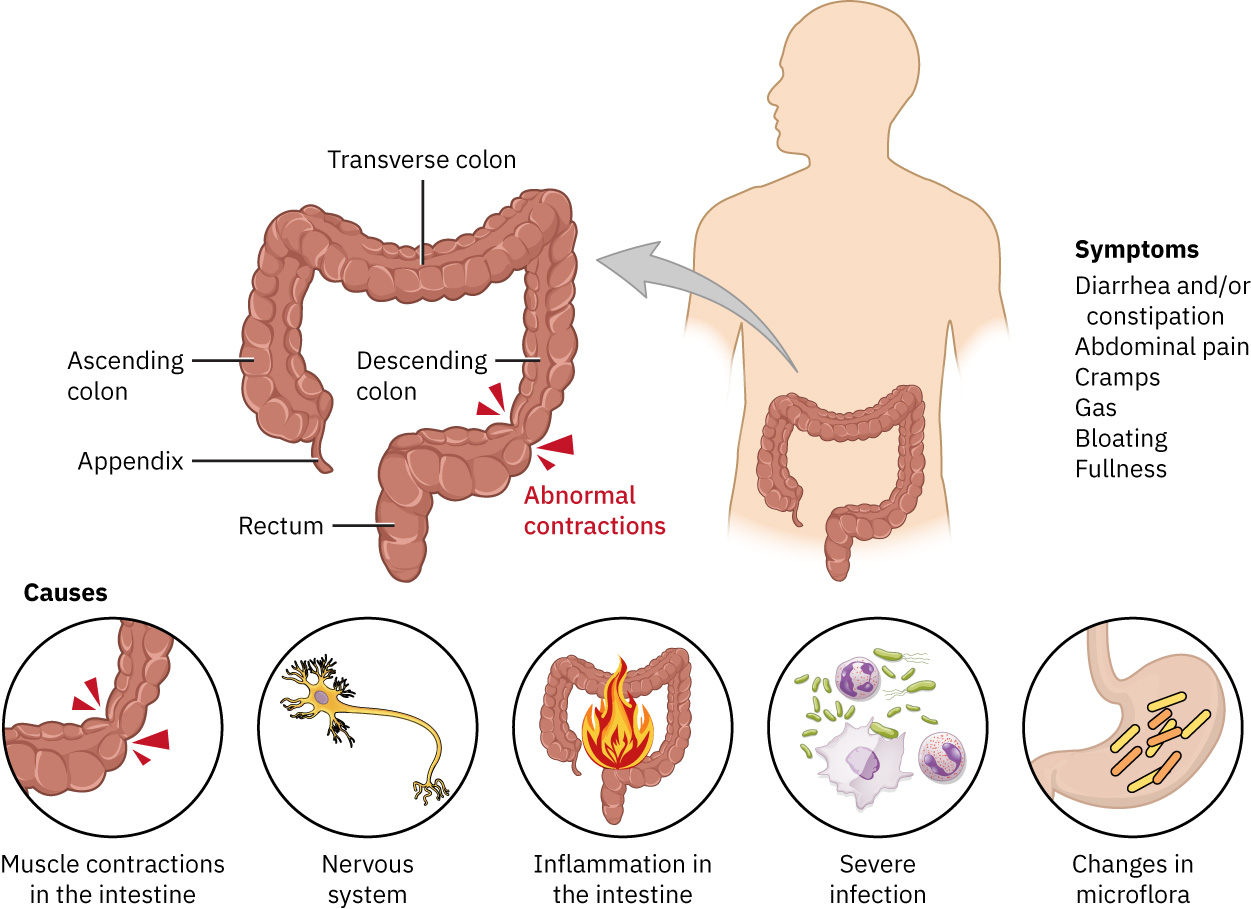 Illustration reference: OpenStax Medical-Surgical Nursing Ch.19.5.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.19.5.
Proposed contributing mechanisms include altered intestinal microbiota, immune-response changes, and environmental stressors such as early-life stress, prior antibiotic exposure, postinfectious changes after gastroenteritis, and food intolerance patterns.
Classification
- IBS-C: Constipation-predominant stool pattern.
- IBS-D: Diarrhea-predominant stool pattern.
- IBS-M: Mixed/alternating constipation and diarrhea pattern.
Nursing Assessment
NCLEX Focus
Distinguish functional IBS patterns from red-flag findings that require evaluation for other GI disease.
- Assess abdominal pain pattern, bowel frequency/consistency, bloating, and trigger-food association.
- Clarify whether pain increases when bowel habits change and improves after bowel movements, which supports an IBS symptom pattern.
- Apply clinical symptom criteria (Rome IV): recurrent abdominal pain at least 1 day/week over 3 months associated with bowel-movement improvement, altered stool frequency, and/or altered stool form.
- Screen psychosocial contributors such as stress, anxiety, and depression burden.
- Monitor hydration and nutrition status when diarrhea or poor intake is present.
- Ask about mucus in stool history and stool amount/frequency trends to refine subtype pattern and trigger review.
- Escalate for alarm features (for example iron-deficiency pattern, hematochezia, unintentional weight loss, or strong cancer/IBD family history) that warrant additional workup.
Diagnostics:
- No single diagnostic test confirms IBS.
- Without alarm findings, diagnostic testing is often minimized; CBC/CMP and stool testing are used selectively to rule out alternative causes when concerning cues are present.
- Colonoscopy may be indicated in selected patients (for example concerning history or risk profile).
- Serum studies may be used to exclude infection or other disease when symptoms are atypical or persistent.
Nursing Interventions
- Guide individualized lifestyle changes: increase activity and reduce trigger foods.
- Use food and symptom diaries to identify personal intolerance patterns and stool trends.
- Reinforce stress-management strategies (for example breathing exercises and meditation) to reduce flare intensity.
- Coordinate referrals to gastroenterology and dietetics for individualized long-term plans.
- Track stool pattern and response to therapy in subtype-specific care (IBS-C vs IBS-D vs IBS-M).
- Prevent dehydration in diarrhea-predominant episodes with oral or IV rehydration as indicated.
- Monitor for escalation cues (for example fever, lethargy, tachycardia, or worsening anxiety with symptom progression) and coordinate prompt provider reassessment.
- Evaluate outcomes with patient-reported symptom burden, fluid-balance stability, and reduced reliance on pain medication when symptoms improve.
Functional Diagnosis, Real Symptoms
IBS is functional rather than structural, but symptom burden can be significant and chronic. Avoid dismissing symptoms; focus on symptom relief and quality-of-life outcomes while screening for red flags.
Pharmacology
| Symptom Pattern | Drug Class | Examples | Key Nursing Considerations |
|---|---|---|---|
| IBS-C | laxatives and fiber support | Psyllium, osmotic/stimulant laxatives (as ordered) | Titrate to stool response; monitor bloating and cramping. |
| IBS-D | antidiarrheals +/- probiotics | Loperamide; selected probiotic strategies | Confirm absence of infectious red flags before routine antidiarrheal use. |
| Severe global symptoms | antidepressants | Low-dose TCAs or SSRIs | May reduce pain and bowel symptom burden; monitor adverse effects and mood status. |
| Selected IBS-D cases | Serotonin-modulating and gut-directed agents | Alosetron (women with IBS-D), rifaximin | Reserve for specific indications; monitor response and adverse effects closely. |
Clinical Judgment Application
Clinical Scenario
A 34-year-old patient reports recurrent crampy abdominal pain and alternating constipation/diarrhea for several months, worsened during high stress, with no bleeding or weight loss.
- Recognize Cues: Chronic recurrent pain, mixed stool pattern, stress linkage, no alarm bleeding/weight loss.
- Analyze Cues: Pattern fits possible IBS-M rather than acute infection or overt inflammatory disease.
- Prioritize Hypotheses: Priority is symptom control with trigger identification and hydration/nutrition protection.
- Generate Solutions: Start food/stool diary, teach stress-management tools, and align subtype-specific symptom medication plan.
- Take Action: Implement education, monitor stool/pain trends, and coordinate GI/dietitian follow-up.
- Evaluate Outcomes: Lower pain scores, improved stool regularity, and fewer activity-limiting flares.
Related Concepts
- constipation - Constipation-focused assessment and staged bowel-regimen interventions.
- diarrhea-assessment-and-management - Diarrhea-focused hydration, infection, and skin-protection priorities.
- antidiarrheals - Drug-class safety and contraindication profile for diarrhea episodes.
- laxatives - Pharmacologic support options for constipation-predominant symptoms.
- inflammatory-bowel-disease - Important inflammatory differential when alarm features are present.
- stress-and-anxiety - Stress-load assessment and nonpharmacologic coping strategies.
Self-Check
- Which symptom features support IBS diagnosis under Rome IV criteria?
- Which alarm findings should prompt workup for diagnoses other than IBS?
- How does treatment differ between IBS-C and IBS-D patterns?