Vascular Access Device Selection and Central Line Safety
Key Points
- Device choice should match therapy duration, solution properties, vein condition, and patient status.
- PIVCs are short-term options, while midline and central access support longer or higher-risk therapies.
- CVC types (PICC, tunneled, nontunneled, implanted ports) have distinct indications and risk profiles.
- Insertion planning should include patient-specific vein-preservation concerns (for example end-stage renal disease) and expected complication risk by site.
- Central-line infection prevention and verification protocols are essential to reduce severe harm.
Pathophysiology
Vascular access introduces a foreign device into the bloodstream pathway. Mechanical trauma, chemical irritation, and microbial entry can cause local and systemic complications. Risk increases when device type does not match therapy intensity or duration.
Central access improves delivery of vesicants, high-osmolar solutions (including hypertonic fluids and total parenteral nutrition), and long-term therapies, but carries higher bloodstream infection and thrombosis risk if insertion and maintenance standards are not followed.
Classification
- Peripheral IV catheter (PIVC): Short-term peripheral access for many fluids and medications; commonly single lumen and often about 3/4 to 1 in length.
- Midline catheter: Longer peripheral option (days to weeks, often 14 days or longer), commonly ultrasound-guided (often 16-18 gauge), with tip in upper-arm vasculature near axillary level; not a central line.
- Central venous catheter (CVC): Central access for high-risk infusates, hemodynamic monitoring, and prolonged therapy.
- Common CVC forms: PICC, tunneled catheter, nontunneled catheter, and implanted port.
- Tunneled CVC profile: External segment with subcutaneous tunnel and cuff (for example Hickman/Permacath), often used for months to years in long-term therapies such as chemotherapy, prolonged antibiotics, or hemodialysis.
- Nontunneled CVC profile: Rapid temporary central access for emergent resuscitation/medication delivery or urgent CVP monitoring; higher infection/dislodgement risk because no tunneled tract/cuff.
- Implanted port profile: Fully subcutaneous access reservoir (typically Huber/noncoring needle access when needed) suitable for intermittent long-term therapy such as chemotherapy, prolonged antibiotics, frequent blood draws, or radiation; reduced external-infection exposure when de-accessed but may involve access discomfort and local scarring.
- Common lumen role pattern for multilumen CVCs: Proximal or middle lumens are frequently used for medications/fluids and parenteral nutrition, while larger distal lumens are commonly prioritized for blood administration, blood sampling, and CVP monitoring per policy.
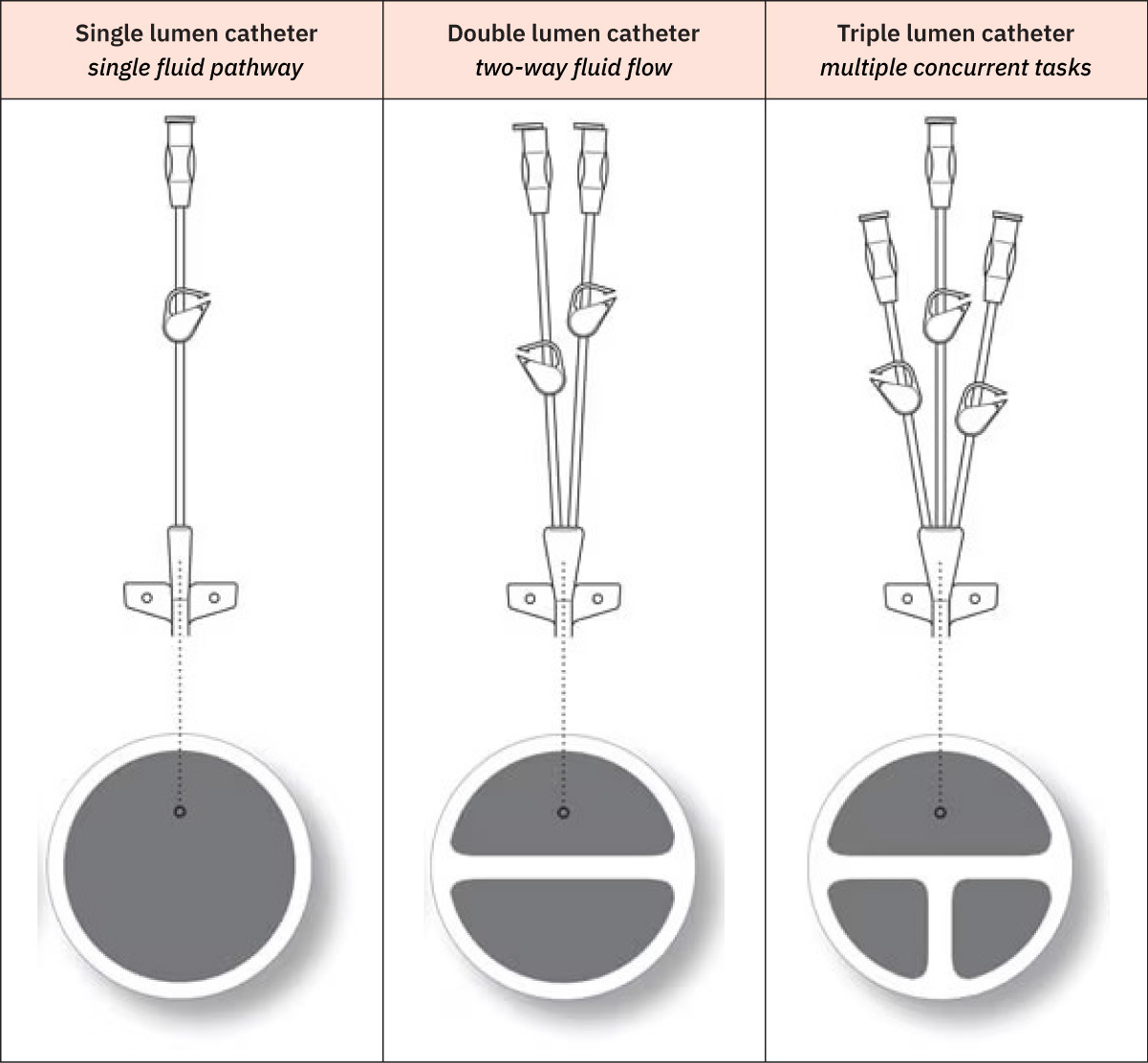 Illustration reference: OpenStax Clinical Nursing Skills Ch.10.
Illustration reference: OpenStax Clinical Nursing Skills Ch.10.
Nursing Assessment
NCLEX Focus
Prioritize matching therapy requirements to the safest viable access route, then monitor line integrity and infection cues continuously.
- Review therapy plan: expected duration, infusion rate, vesicant potential, osmolarity, and need for multiple lumens.
- Assess vein quality, prior access history, mobility impact, and limb restrictions.
- For midline planning, verify that intended infusates are appropriate for peripheral-depth delivery (for example avoid TPN and other high tissue-injury solutions per policy).
- Identify limb restrictions before insertion attempts (for example limb-alert status, mastectomy/lumpectomy side, AV fistula, lymphedema, DVT, fracture, or major contracture/scarring).
- Assess for vein-preservation priorities (for example dialysis-fistula planning in end-stage renal disease) that can make PICC placement less appropriate.
- Confirm insertion-site appropriateness and line-position verification where required (for example fluoroscopy during insertion or post-procedure chest X-ray when fluoroscopy is not used).
- Reassess at least once per shift in acute care (and as needed by status/policy): insertion site plus adjacent neck/chest/extremity skin, dressing integrity, catheter function, and early signs of infiltration, phlebitis, thrombosis, or infection.
- For tunneled lines, include tract-area pain, swelling, drainage, and erythema checks.
- For tunneled externalized lines, reinforce site-dry precautions during bathing and assess securement integrity at both exit and tunnel-related areas.
- Trend catheter external length against baseline and monitor PICC arm circumference each shift; measuring about 10 cm above the antecubital fossa and noting an increase around 3 cm can indicate edema with possible DVT.
- Confirm all infusing fluids/medications are labeled and verify Luer-lock connections remain secure to reduce contamination, leakage, and air entry risk.
Nursing Interventions
- Escalate from PIV to midline or central access when therapy profile exceeds peripheral safety limits.
- Reevaluate access strategy when IV therapy duration extends beyond about six days, with consideration for intermediate or long-term devices.
- For rapid peripheral infusions, preferentially evaluate larger upper-arm veins (cephalic, basilic, brachial) over smaller hand veins when clinically appropriate.
- Use ultrasound-guided insertion support for peripheral and central devices when available to improve first-attempt success and reduce complications.
- Ensure central-line insertion is performed by appropriately credentialed personnel; noninserter nurses support sterile setup and procedural assistance.
- Use engineered securement (suture or sutureless by device/policy) to minimize dislodgement, vessel injury, and therapy delays.
- Use aseptic insertion/maintenance workflows and standardized line-access disinfection.
- Apply line-specific flushing, tubing-change, and dressing-change protocols.
- Promptly report and intervene for suspected CLABSI, catheter-associated thrombosis, or extravasation.
- Recognize central-line-specific insertion/maintenance risks including pneumothorax, accidental line removal with hemorrhage risk, and air embolism.
- Minimize unnecessary CVAD access/manipulation episodes to reduce contamination opportunities.
- Decontaminate needleless hubs/connectors with vigorous friction scrub (typically at least 15 seconds and up to about 60 seconds; scrub top and sides) or use approved antiseptic protective caps per policy.
- For suspected catheter occlusion, assess for blood return and infusion resistance; never flush against resistance, check for kinks, and attempt positional maneuvers (arm elevation, cough/deep breathing, posture change) before escalation.
- To reduce catheter breakage risk, use a 10-mL syringe for flushing, avoid sharp objects near tubing, and clamp with sterile gauze near the insertion site if a break is identified while awaiting repair/replacement.
- Flush per policy after insertion-tip verification, before/after infusions, and before/after blood sampling; consider flushing all lumens after blood draws in multilumen devices to reduce blood reflux.
- For inactive lines, use maintenance flush/lock schedules per policy (commonly around every 7 days for unused CVADs; implanted ports are commonly maintained about every 4 weeks, with some policies using 4 to 6 week ranges).
- Use pulsatile flushing and lumen-appropriate volume targets (often around twice lumen volume), and attempt blood aspiration before flush to confirm patency.
- Follow connector-specific clamping sequence (negative vs positive vs neutral needleless connectors) to reduce reflux risk.
- For IVAD access, disinfect skin with chlorhexidine and allow to dry, use a noncoring needle, and verify whether the port is power-injectable before CT contrast use; if status is unknown, treat as nonpower-injectable.
- Before IVAD access, confirm tip-placement documentation, verify antiseptic/anesthetic/solution allergies, assess overlying skin and device rotation, and select the smallest noncoring needle gauge/length that supports prescribed therapy.
- For implanted ports under active access, follow policy/manufacturer frequency for flush and needle changes (for example flush at least daily when indicated and re-access/change needle about every 7 days).
- Use sterile-field technique to prime extension/connector before puncture, insert the noncoring needle perpendicular through the septum until seated, verify blood return/low-resistance flush, then secure while preserving site visibility.
- Trend and document catheter external length to detect dislodgement/migration; do not readvance an externally migrated line, and if complete dislodgement occurs, cover the site, apply direct pressure, and activate rapid response support.
- Prevent air embolism by keeping hubs closed and clamps engaged; if suspected, stop further air entry, call rapid response, administer high-flow oxygen, and position left-side head-down per policy.
- If incorrect placement or insertion-related pneumothorax is suspected, stop infusions and escalate immediately for imaging/provider intervention.
- For PICC-specific protection, avoid venipuncture/peripheral cannulation/BP measurement on the PICC arm, keep dressing dry, and avoid tight elastic coverings that increase thrombosis/phlebitis risk.
- For PICC care, reinforce “keep dry” precautions during bathing and perform flushes before/after use plus maintenance flushes per policy to preserve patency.
- For tunneled CVC care, flush before/after use and on maintenance schedule per policy, and confirm lumen-specific line-use plans when multiple lumens are present.
- Include site-assessment teaching for home/outpatient clients and caregivers (inspection frequency, warning signs, and when to notify the provider).
- Reassess daily whether the CVAD remains necessary and escalate removal when no longer indicated.
- For emergently placed nontunneled CVCs, anticipate early transition/removal planning (often within about 48 hours per policy/guideline context) once stable alternative access is available.
- During ongoing infusion therapy, trend cardiopulmonary status, intake/output, daily weight, and relevant laboratory values to detect early complications.
- Before discharge with IVAD/CVAD, confirm patient/caregiver device-management readiness and coordinate home-health follow-up plus supplies (dressings, flushes, and tubing) as needed.
- For IVAD access events, include documentation of needle gauge/length, number of access attempts, flush type/amount, patency and blood-return findings, tolerance, teaching, and any unexpected outcomes/interventions.
Device-Therapy Mismatch Risk
Using inadequate access for vesicants or prolonged high-risk infusions increases tissue injury and infection risk.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| vesicants | Vancomycin, dopamine, phenytoin | Prefer larger or central access when indicated; monitor closely for tissue injury cues. |
| antibiotics | Broad-spectrum IV agents | Long-course therapy may require durable access and strict line-infection prevention. |
Clinical Judgment Application
Clinical Scenario
A patient with fragile veins needs two weeks of IV antibiotics and intermittent vesicant therapy.
- Recognize Cues: Repeated peripheral failures with planned prolonged treatment.
- Analyze Cues: Ongoing PIV attempts increase trauma and therapy interruptions.
- Prioritize Hypotheses: Device upgrade is needed to reduce complications and preserve treatment reliability.
- Generate Solutions: Collaborate for midline or central access based on medication profile and duration.
- Take Action: Implement line-care bundle and monitor for early complications.
- Evaluate Outcomes: Infusions proceed reliably with reduced access-related events.
Related Concepts
- peripheral-iv-access - Initial peripheral access principles and site selection.
- iv-insertion-and-iv-removal - Practical insertion/removal workflow and safety checks.
- peripheral-iv-therapy-complications - Local/systemic complication cues and escalation.
- catheter-related-bloodstream-infection - Bloodstream infection prevention and response priorities.
- infiltration-and-extravasation - Tissue injury recognition and immediate intervention pathway.
Self-Check
- Which factors should trigger escalation from peripheral to central access?
- Why are midlines not appropriate for certain high-risk infusates?
- Which daily checks reduce central-line complication risk most effectively?