Leadership Attributes and Competencies in Nursing
Key Points
- Effective nurse leadership is behavior-based influence, not title-based authority.
- Effective leadership empowers others toward shared goals rather than relying on command-and-control behaviors.
- Competencies are commonly organized as leading self, leading others, and leading the organization.
- High-impact attributes include commitment to excellence, commitment to profession, integrity, accessibility, creativity, problem-solving, adaptability, and communication.
- Effective leaders consistently demonstrate integrity, courage, initiative, disciplined energy use, optimism, perseverance, healthy balance, stress management, and strong communication.
- Closed-loop communication and structured handoff frameworks (for example ISBAR and I-PASS) improve reliability during transitions and urgent care.
- Leadership quality directly affects team culture, patient safety, and care outcomes.
- Nursing leadership includes bedside clinical leadership, not only formal administrative roles.
- Team leadership is dynamic; the member with the most relevant expertise may temporarily lead a task while team accountability remains shared.
- TeamSTEPPS leadership methods use pre-brief and debrief checklists to improve coordination and continuous improvement.
- Entry-level RNs demonstrate leadership through daily prioritization, interprofessional coordination, discharge-resource linkage, practice-improvement participation, and learner support.
- Effective followership strengthens leadership by using upward influence, situational awareness, and timely speaking-up to protect patient safety.
- ANA Leadership is a professional performance expectation for all RNs, even when they are not serving in formal manager roles.
- Effective team leadership includes shared accountability with clients/communities, structured reflection on team performance, and process-improvement actions across diverse care settings.
- TeamSTEPPS organizes teamwork into team structure plus four core skills: communication, leadership, situation monitoring, and mutual support.
Pathophysiology
Nursing leadership functions as a systems-level safety mechanism. Weak leadership behaviors can amplify communication failures and delay escalation, while strong leadership improves coordination, accountability, and patient-centered execution.
Competency-driven leadership supports consistency across routine care and high-acuity events by aligning individual actions with team and organizational goals.
Leadership is behavior-driven and not limited to formal management titles, so bedside nurses can exert leadership influence through consistent actions.
Classification
- Leading self: Self-awareness, responsibility, accountability, initiative, and integrity.
- Leading others: Communication, trust-building, conflict handling, mentorship, and respect.
- Leading organization: Change leadership, systems thinking, decision-making, and strategic vision.
- Systems-leadership triad: Individual collaborative-leadership behaviors, community coalition/advocacy tactics, and system-level understanding of complex drivers of care outcomes.
- Followership domain: Upward influence through proactive engagement, constructive communication, collaboration, ethical advocacy, and continuous improvement.
- IPEC teams/teamwork behavior domain: Relationship-building, team-role adaptability, constructive disagreement management, shared outcome accountability, and routine individual/team performance reflection for improvement.
- Professional-commitment attributes: Commitment to excellence and commitment to profession through quality improvement, evidence-based practice, and policy/professional engagement.
- Attribute layer: Integrity, courage, initiative, energy stewardship, optimism, perseverance, balance, healthy stress handling, and ethical reliability.
- Team-leadership tools domain: Brief checklists, debrief checklists, plan monitoring, change communication, and mutual-support prompting.
- TeamSTEPPS skill domain: Team structure, communication, leadership, situation monitoring, and mutual support.
- Leadership-task cycle domain: Share plan (brief), monitor/modify plan (huddle), and review performance (debrief).
Nursing Assessment
NCLEX Focus
Leadership questions often test which competency domain is most needed for a specific unit problem.
- Assess whether leadership gaps are at self, team, or system level.
- Assess communication reliability during handoffs and acuity changes.
- Assess whether sender-receiver confirmation and check-back are consistently used for critical tasks.
- Assess team trust, psychological safety, and conflict patterns.
- Assess alignment between unit behaviors and facility values.
- Assess leader visibility and accessibility during operational stress.
- Assess ability to reprioritize staffing roles quickly during surge or shortage events without losing communication reliability.
- Assess whether teams consistently use pre-brief/debrief routines to align plans and learn from outcomes.
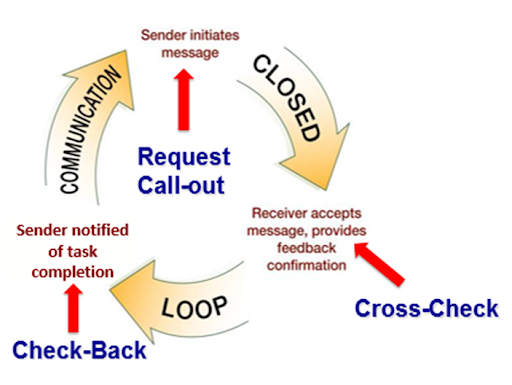 Illustration reference: OpenRN Health Alterations Ch.1.2.
Illustration reference: OpenRN Health Alterations Ch.1.2.
Nursing Interventions
- Use domain-based self-audit to target leadership growth priorities.
- Implement structured team communication and debrief routines.
- Use daily huddles when role confusion or missed tasks emerge to clarify responsibilities and surface concerns early.
- Use closed-loop communication for urgent orders and high-risk delegated tasks.
- Build followership reliability by explicitly inviting concerns, rewarding respectful challenge, and requiring message confirmation for safety-critical communication.
- Use brief checklists at project or shift start to align goals, role ownership, and contingency plans.
- Use debrief checklists at project or shift end to capture successes, defects, and next-cycle adjustments.
- At shift start, run a brief that confirms team membership, goals, roles, highest-acuity clients, workload distribution, and available resources.
- During change in unit conditions, run huddles to refresh situational awareness and reassign tasks/resources.
- After significant events (for example code/emergent response), run debriefs focused on communication clarity, role execution, workload equity, errors avoided/made, and next-cycle improvements.
- Provide constructive feedback in private using specific observations, clear impact statements, and practical coaching steps.
- Model transparent error reporting and ethical decision pathways.
- Maintain approachable leadership presence (for example open-door access and routine rounds) so staff escalate concerns early.
- Lead quality-improvement and evidence-based-practice adoption efforts to normalize a unit culture of excellence.
- Model work-life boundaries and practical stress-management behaviors so team members can sustain performance.
- Build mentorship touchpoints for less-experienced staff.
- Identify emerging leaders and assign mentored project leadership opportunities to strengthen succession planning.
- Pair quality goals with measurable behavior expectations.
- Project leadership from any role by mentoring, participating in committees, and engaging in community or policy-focused professional activities.
- Operationalize ANA leadership competencies in daily practice: lead decision-making discussions, build interprofessional trust, communicate for change and conflict resolution, and maintain delegation accountability.
- Use systems-leadership framing during change projects: define individual role behaviors, community/stakeholder alignment actions, and system-level barriers/enablers before implementation.
Title-Without-Influence Risk
Positional authority without relational trust can reduce follow-through during safety-critical events.
Pharmacology
Leadership competency affects medication safety through supervision quality, role clarity, and timely escalation when adverse responses occur.
Clinical Judgment Application
Clinical Scenario
During a short-staffed shift, bedside communication becomes fragmented and near-miss events increase.
- Recognize Cues: Unit issues involve trust, communication, and role confusion.
- Analyze Cues: Deficits span leading others and leading organization domains.
- Prioritize Hypotheses: Team communication redesign is urgent.
- Generate Solutions: Standardize huddles, escalation scripts, and mentorship support.
- Take Action: Implement structured role check-ins and safety rounds.
- Evaluate Outcomes: Fewer near misses and improved team reliability.
Related Concepts
- leadership-styles-and-situational-use-in-nursing - Links competency to style selection.
- management-functions-and-structures-in-nursing - Connects influence to operational execution.
- nursing-advocacy-in-professional-practice - Leadership as patient and workforce advocacy in action.
- isbar-clinical-handoff-communication - Structured handoff and readback practices that operationalize leadership communication.
Self-Check
- Which leadership domain is most relevant when unit morale declines?
- Why does accessibility improve safety in high-acuity settings?
- How does integrity influence delegation and supervision quality?