Ethical Theories and Approaches in Nursing
Key Points
- Nursing ethics draws from multiple theories rather than a single model.
- Virtue ethics focuses on character; deontology focuses on duty; utilitarianism focuses on outcomes.
- Principle-based approaches are widely used and often dominant for bedside nursing decisions.
- Care-based and feminist ethics highlight dependency, relationships, power, and justice.
- RN duty language in nurse-client relationships is commonly deontological, especially around beneficence and nonmaleficence.
- Utilitarian reasoning supports society-level resource allocation but can conflict with individual rights and justice.
- Public-health ethics often requires explicit rights-balancing tests: necessity, reasonable means, proportionality, and minimizing individual harm.
- Different ethical frameworks can produce the same clinical decision while using different rationale (duty vs outcome).
- An ethical dilemma reflects competing values with no clearly superior option; a moral dilemma reflects known right action constrained by external barriers.
- Structured RN frameworks include nursing-process ethics mapping, the four-quadrant approach, the MORAL model, and the PLUS decision model.
- A CJMM-based ethics workflow can operationalize decisions by pairing cue analysis with legal, cultural, and principle-based checks.
Pathophysiology
Complex clinical dilemmas often involve competing goals, unequal power, and uncertain outcomes. Ethical theory provides structured reasoning to reduce inconsistent decisions and improve fairness, safety, and transparency in care.
Classification
- Virtue ethics: Right action emerges from good moral character.
- Deontology: Right action follows moral law and duty regardless of outcome.
- Clinical-duty deontology: In nurse-client care, duty-oriented obligations center on doing good and avoiding harm.
- Utilitarianism: Right action seeks greatest good and least harm for the most people.
- Resource-allocation utilitarianism: Uses finite system resources (time, money, staffing, treatment access) for population-level benefit.
- Principle-based approach: Uses ethical principles as direct guides for nursing action and aligns closely with code-based clinical reasoning.
- Care-based approach: Emphasizes caring relationships, vulnerability, and authentic response.
- Care-based nursing ethics: Uses holistic, situation-specific analysis instead of rigid prefabricated rule application.
- Feminist ethics: Examines power, oppression, and inequity in healthcare relationships.
- Decision-process models: Structured tools such as the MORAL model support stepwise choice in complex ethical dilemmas.
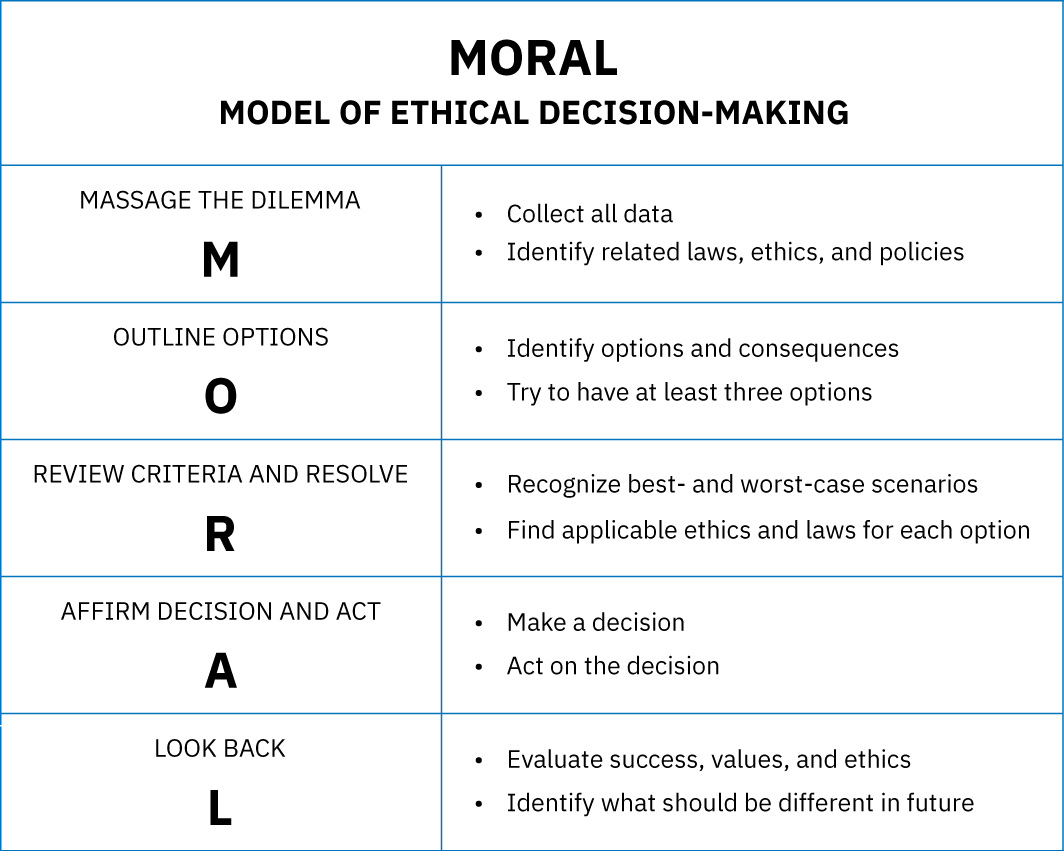 Illustration reference: OpenStax Fundamentals of Nursing Ch.16.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.16.2. - Four-topics approach: Team-based framing through medical indications, patient preferences, quality of life, and contextual features.
- Ethical dilemma: Conflict between competing values with no clearly superior choice.
- Moral dilemma: The ethically right action is identified, but practical or organizational constraints block execution.
- Nursing-process ethics model: Uses assessment/data collection, analysis, diagnosis, outcomes, planning, implementation, and evaluation to resolve ethical issues.
- CJMM ethics sequence: Recognize/analyze ethical cues, prioritize/generate options using legal and principle checks, take action with consequence testing, and evaluate ethical justification.
- PLUS model: Organization-focused ethical filter set using policies, laws, universal values, and self-identification of what is right and fair.
- Public-health rights-balancing domain: Restrictive interventions should meet necessity, reasonable means, proportionality, and harm-minimization standards.
Nursing Assessment
NCLEX Focus
Questions often test which ethical framework best explains a decision rationale in a specific case.
- Assess whether the dilemma is primarily duty-based, outcome-based, or relationship-based.
- Assess where autonomy, justice, and harm-prevention conflicts are strongest.
- Assess whether vulnerability or power imbalance should change the reasoning lens.
- Assess team assumptions that may reflect bias or unequal voice distribution.
- Assess whether a single framework is sufficient or blended reasoning is needed.
- Assess whether culture-based family-centered disclosure preferences conflict with U.S. HIPAA requirements and client autonomy.
- Assess ANA ethical-competence factors: personal-value appraisal, code-awareness, principle knowledge, and readiness to implement decisions.
- Assess whether unresolved uncertainty has progressed from moral conflict to moral distress or moral outrage.
Nursing Interventions
- State the guiding framework explicitly during team ethical discussion.
- Use principle-based checks for bedside decisions with immediate patient impact.
- Add care-based analysis when relational trust and vulnerability are central.
- Apply feminist ethics when inequity, bias, or structural barriers shape options.
- Use a structured sequence (for example MORAL: massage, outline, review, affirm/act, look back) when options are closely contested.
- Use four-topics team review when ethical disagreement persists across disciplines.
- Use nursing-process ethics mapping to keep analysis explicit: define issue and stakeholders, identify value conflicts, set autonomy-aligned goals, choose feasible options, implement collaboratively, and evaluate learning.
- In CJMM-based ethics decisions, include procedural conflicts, decision-capacity review, legal directives (for example DNR), stakeholder values, and anticipated consequences before choosing an option.
- Use PLUS filters when policy/legal/organizational constraints are central, then apply the seven-step PLUS sequence to test alternatives before final action.
- In population-level restrictions, apply necessity-proportionality-harm-minimization checks and keep decisions science-based, community-specific, and transparent with two-way communication.
- When family-centered nondisclosure norms are present, escalate early for ethics consultation and align communication with law and policy.
- Document ethical rationale to support continuity and accountability.
Framework Blind Spot
Using only one ethical lens can hide key risks, especially power imbalance and inequity factors.
Pharmacology
Medication ethics may require combined reasoning: duty to informed consent (deontology), harm minimization (utilitarian), and patient-centered relationship factors (care-based approach).
Clinical Judgment Application
Clinical Scenario
A team debates a high-burden intervention with low expected benefit for a frail patient who prioritizes comfort.
- Recognize Cues: Outcome uncertainty and preference conflict are present.
- Analyze Cues: Utilitarian and autonomy considerations are both highly relevant.
- Prioritize Hypotheses: Principle-based and care-based reasoning together may be most balanced.
- Generate Solutions: Compare options through benefit-harm, duty, and relational impact lenses.
- Take Action: Present a patient-aligned plan with explicit ethical rationale.
- Evaluate Outcomes: Care remains ethically coherent and goal-concordant.
Related Concepts
- nursing-ethical-principles-and-virtues - Foundational principles and virtues used across frameworks.
- nursing-advocacy-in-professional-practice - Advocacy as an ethical action pathway.
- quality-improvement-nurse-role-and-qapi - System-level context for justice and equity concerns.
Self-Check
- What is the practical difference between deontological and utilitarian reasoning?
- When is care-based ethics especially useful in nursing decisions?
- How does feminist ethics strengthen analysis of healthcare inequity?