Disaster Preparedness Response and Recovery in Community Health Nursing
Key Points
- Disaster management integrates preparedness, mitigation, response, and recovery in a continuous cycle.
- RN disaster planning must include social vulnerability analysis because catastrophic impact is not distributed equally across populations.
- Response operations prioritize lifesaving care, shelter/food/water access, and early psychological stabilization.
- Field triage and disaster triage (for example START) allocate limited resources during surge events.
- Chemical and environmental exposure events require rapid contamination-risk assessment and decontamination decisions to prevent secondary harm.
- Recovery extends beyond infrastructure repair and requires monitoring for PTSD, substance-use escalation, and suicide risk.
- Disaster readiness depends on a prepared nursing workforce that includes active, reserve, retired, and volunteer nurses across civilian and uniformed systems.
- Environmental disasters include weather- and geologic-hazard pathways (for example floods, hurricanes, tsunamis, earthquakes, landslides, and wildfires) that can rapidly block access to care.
- Biological disasters include infectious outbreaks, pandemics, and deliberate biologic release events that require rapid surveillance and infection-control escalation.
- Technological disasters include chemical, radiological, nuclear, and cyber/infrastructure failures that can rapidly disrupt both patient safety and care delivery systems.
- Bioterror readiness requires early recognition of unusual exposure signals and rapid reporting through local health-department and CDC/public-health channels.
- Epidemic and pandemic response requires early pattern recognition (point-source, propagated, mixed transmission), rapid triage/isolation, and sustained community risk communication.
- Outbreak communication effectiveness is strongly influenced by perceived risk factors and the communicator’s trustworthiness.
- Historical pandemic patterns show that early, consistent nonpharmacologic interventions and adequate nursing workforce capacity strongly affect mortality trajectories.
- Pandemic response quality declines when stigma drives delayed care, inequitable treatment access, or mistrust in affected communities.
- Community disaster resilience depends on coordinated phase-based action (mitigation, preparedness, response, recovery) and culturally inclusive planning.
- Hospital preparedness depends on recurring disaster training, performance evaluation, and role clarity within an incident command structure.
- Mass-casualty triage tags align urgency with resource limits and require rapid reassessment as patient condition and capacity change.
- Hospital readiness during disasters depends on surge-capacity expansion, infection-control containment, and reliable internal/external emergency communication.
- Mass-violence incidents (for example active-shooter and terrorism events) create broad psychosocial injury and fear burden that extends beyond direct casualties.
Pathophysiology
Disasters create combined physical, environmental, and psychological injury load at a population scale. Health impact is driven by exposure intensity, baseline community vulnerability, and local response capacity.
Nursing outcomes worsen when preparedness and coordination are weak. Early organization of communication pathways, triage, hazard control, and behavioral health support reduces avoidable morbidity and mortality.
Classification
- Preparedness: Pre-event planning, risk mapping, training, and education for likely hazards.
- Mitigation: Actions that reduce hazard probability and downstream severity before impact.
- Response: Immediate post-event lifesaving operations, stabilization, and essential-needs support.
- Recovery: Long-duration restoration of services, infrastructure, and psychosocial function.
- Community-response-phase domain: Phase-based cycle of mitigation, preparedness, response, and recovery used to organize local disaster action.
- Social-vulnerability domain: Community characteristics (for example poverty, transport barriers, crowding, age/disability concentration) that increase disaster risk and slow recovery.
- Triage domain: Field triage/disaster triage processes used to prioritize limited treatment and transport capacity.
- Triage-tag domain: Color-coded class assignment (red immediate, yellow urgent, green delayed/ambulatory, black expectant) used to direct scarce resources under mass-casualty standards.
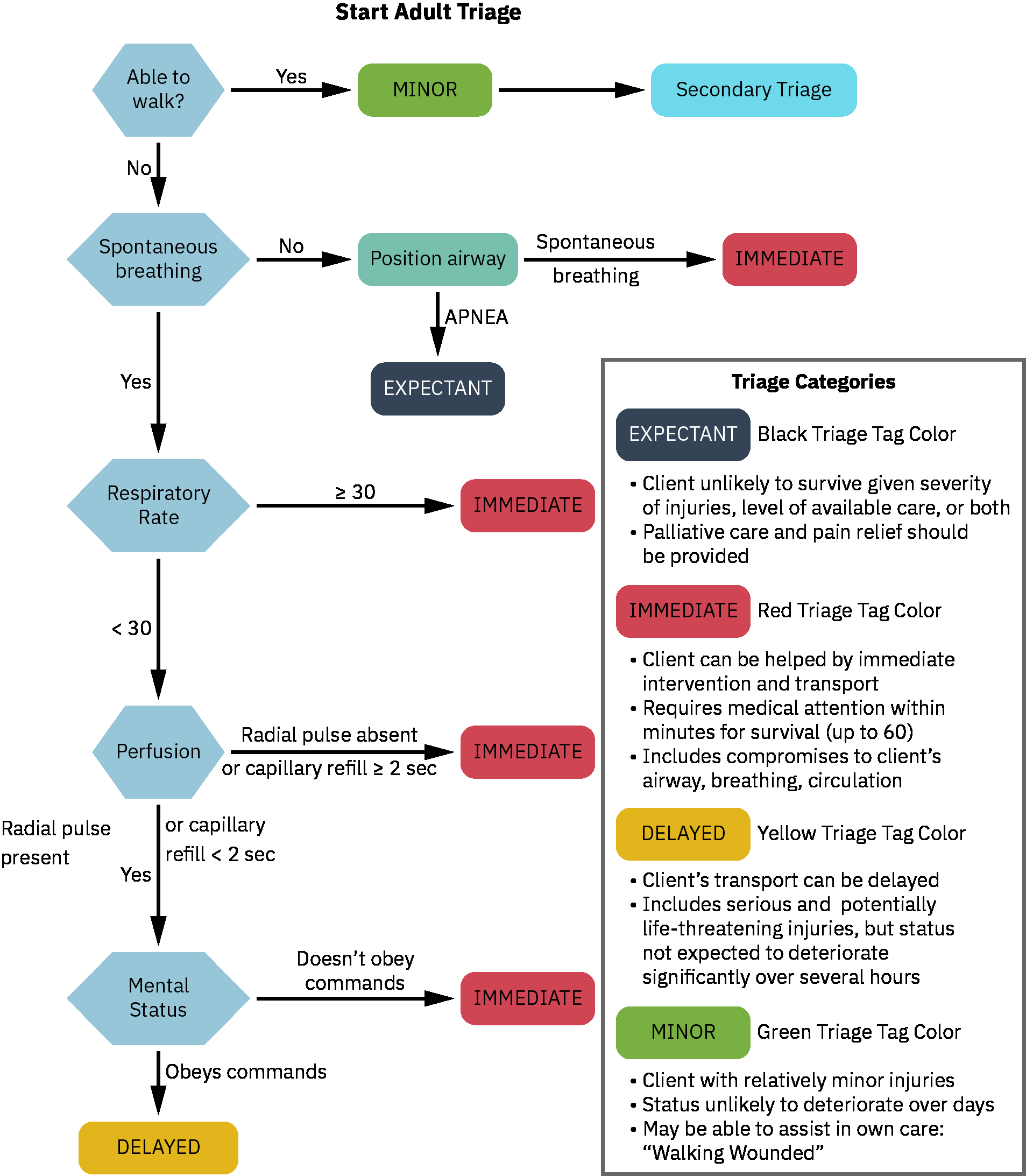 Illustration reference: OpenStax Population Health for Nurses Ch.32.5.
Illustration reference: OpenStax Population Health for Nurses Ch.32.5.
- Hazard-exposure domain: Chemical, biologic, and environmental exposures requiring contamination control and targeted treatment pathways.
- Environmental-hazard domain: Water-related disasters (storm surge, flash flooding, snowmelt flooding, tsunami) and land-related disasters (earthquake, landslide, wildfire) that create different evacuation and infrastructure-failure patterns.
- Weather-alert domain:
watchindicates favorable conditions;warningindicates imminent or ongoing hazard requiring immediate protective action. - Biological-disaster domain: Infectious disease outbreaks, pandemics, and bioterrorism scenarios requiring syndromic surveillance, case reporting, and surge infection-control operations.
- Bioterror-mass-exposure domain: Early recognition, PPE-protected assessment, decontamination-zone setup, command communication, and rapid triage/transport reduce secondary spread and mortality.
- Federal-countermeasure domain: Strategic National Stockpile and medical countermeasures (vaccines, antimicrobials/antivirals/antidotes, diagnostics, and PPE) support short-term surge gaps during public-health emergencies.
- Outbreak-scale domain:
epidemicindicates above-expected regional disease occurrence;pandemicindicates international spread across multiple countries/regions. - Outbreak-pattern domain: Point-source outbreaks (single shared exposure), propagated outbreaks (person-to-person spread), and mixed outbreaks (combined mechanisms).
- Risk-perception determinant domain: Outbreak-message uptake varies by whether risks are viewed as voluntary versus imposed, controllable versus externally controlled, familiar versus novel, and trusted-source versus untrusted-source.
- Risk-communication credibility domain: Empathy/caring, honesty/openness, dedication/commitment, and demonstrated competence increase public adherence.
- Historical-pandemic lesson domain: Prior pandemics repeatedly demonstrate spread through mobility/crowding networks and delayed control when response implementation is fragmented.
- Nonpharmacologic-control bundle domain: Isolation, quarantine, masking, distancing, hygiene/disinfection, and movement restrictions are core controls when vaccines/therapeutics are unavailable or delayed.
- Workforce-surge equity domain: Nursing shortages and inequitable workforce utilization reduce response capacity and worsen outcomes during severe waves.
- Stigma-equity domain: Stigmatizing labels and exclusionary messaging reduce testing, disclosure, treatment engagement, and equitable care access during prolonged infectious crises.
- Prolonged-pandemic management domain: Some pandemics transition into long-duration global burdens requiring sustained surveillance, treatment access, and prevention adaptation rather than short-wave response only.
- High-consequence-outbreak domain: Severe pathogens (for example Ebola virus disease) require strict exposure control, high-level PPE reliability, and protected handling of high-risk body-fluid exposure contexts.
- Technological-disaster domain: Industrial/transport/infrastructure incidents, cyberattacks, and utility failures that may cascade into chemical/radiological exposure and documentation-system downtime.
- Radiological-nuclear domain: Radiation exposure events with acute and delayed morbidity, long-term contamination risk, and sustained public-health monitoring needs.
- Workforce-readiness domain: Staffing and competency capacity across clinical settings, public-health systems, and volunteer response networks.
- Personal-preparedness domain: Individual nurse planning for family communication, transportation access, and role activation expectations during disasters.
- Culture-of-preparedness domain: Multilingual risk communication, culturally appropriate shelter operations, and community-leader engagement to improve trust and participation during crises.
- Hospital-preparedness domain: Facility emergency planning that integrates staff training, competency evaluation, communication pathways, and resource allocation workflows.
- Incident-command domain: Structured command framework that defines roles, reporting, and decision authority during emergency operations.
- NIMS/ICS domain: Multiagency response uses common terminology and defined command roles (incident commander, operations, planning, logistics, finance/administration, liaison, safety, and intelligence/investigation functions).
- Zone-of-care domain: CBRN-capable events may require hot (direct contamination), warm (triage/decontamination), and cold (treatment/holding) zone separation.
- Drill-evaluation domain: Tabletop, simulation, and skills-based drills followed by debrief and corrective-action planning to improve operational readiness.
- Surge-capacity domain: Expansion of care areas, staffing, and supplies to absorb patient volume above normal operations.
- Emergency-communication domain: Policy-driven internal staff communication plus external coordination with families, responders, and community partners during crisis.
- Infection-control-surge domain: Outbreak/disaster containment using isolation precautions, PPE, environmental cleaning, and patient cohorting.
Nursing Assessment
NCLEX Focus
Prioritize immediate life threats first, then assess vulnerability, contamination risk, and behavioral health burden.
- Assess disaster type and likely hazard profile (natural, man-made, infectious, or mixed exposure).
- Assess social vulnerability factors that may limit evacuation, resource access, and recovery capacity.
- Assess local hazard profile and seasonality (for example severe storms, heat burden, wildfire risk, earthquake/landslide exposure, and flood-prone terrain).
- Assess current phase of disaster management to match intervention priorities.
- Assess for early biologic-threat cues (clustered febrile illness, unusual severity patterns, rapid community spread, or atypical exposure history) and report per protocol.
- In possible bioterror contexts, assess sentinel indicators such as unusual dead/dying animals, unexplained severe illnesses/deaths, atypical vapors or odors, and unusual insect swarms.
- Assess probable outbreak pattern and transmission dynamics (shared-source cluster versus sustained person-to-person spread) to guide containment priorities.
- Assess availability of communication, coordination, and collaboration assets among health agencies and community partners.
- Assess whether response plans account for language access, cultural practices, and trusted local leadership needed for equitable emergency communication.
- Assess perceived-risk drivers in the target audience (control, familiarity, expected benefit timing, and trusted messenger).
- Assess nursing workforce readiness, including surge staffing options, role clarity, and just-in-time competency needs for disaster deployment.
- Assess whether surge staffing plans include equitable and full workforce mobilization to prevent avoidable staffing gaps.
- Assess hospital emergency-policy readiness, including incident-command role assignment, internal/external communication flow, and resource-allocation triggers.
- Assess recent drill and debrief findings to identify unresolved competency gaps in triage, communication, and team coordination.
- Assess personal disaster-readiness conflicts for deployed nurses (duty-to-care versus family safety obligations) before events occur.
- Assess triage category and clinical trajectory using established mass-casualty protocols when surge standards are active.
- In mass-violence/MCI response, assess scene-security status first (for example active offender, secondary explosive risk, and collapse/fire hazards) before clinical approach.
- Assess class-specific triage urgency and expected treatment window to prioritize immediate versus delayed care needs.
- Assess whether ambulatory green-tag patients could leave screening areas while still posing contamination risk to other environments.
- Assess for contamination indicators: exposure symptoms, visible residue on skin/clothing, proximity to release site, and detection-device results.
- Assess need for decontamination to protect the patient, staff, first receivers, and surrounding care infrastructure from secondary contamination.
- Assess surge-capacity readiness, including expandable treatment spaces, supplemental staffing plans, and high-volume resource-allocation triggers.
- Assess disaster infection-control readiness (isolation flow, PPE supply, environmental cleaning throughput, and cohorting feasibility) during high census.
- Assess emergency communication reliability for internal command updates and external messaging to patients, families, EMS, and community agencies.
- Assess whether stigma, discrimination, or misinformation is reducing help-seeking, testing uptake, or adherence in affected populations.
- Assess access-to-care disruption risk (blocked roads, damaged facilities, communication failure, electrical power loss, and interruption of home medications/equipment).
- Assess technological-dependency failures (EHR downtime, communication-system compromise, device/equipment malfunction) that can alter triage and medication safety workflows.
- Assess survivor emotional status for fear, anxiety, despair, and functional decline during response and recovery periods.
- In infectious-disease emergencies, assess screening/testing throughput, vaccine-distribution workflow, and transmission-precaution reliability.
- During recovery, assess for delayed behavioral sequelae including PTSD symptoms, substance misuse, and suicide-risk cues.
Nursing Interventions
- Build preparedness plans that integrate hazard analysis, staff training, and community education.
- Use recurring hospital preparedness drills (tabletop, functional, and full-scale multiagency exercises) with post-drill debrief to close identified response gaps.
- Use mitigation planning with the three operational priorities: communication, coordination, and collaboration.
- Implement response actions for lifesaving treatment, basic-needs access, and rapid referral to shelter/resource systems.
- During active response, support command-center communication, emergency-shelter operations, evacuation coordination, and rapid triage for displaced/high-risk populations.
- Integrate weather and hazard intelligence from authoritative public alerts into staffing, evacuation, and shelter-in-place decisions.
- Apply standardized mass-casualty triage systems consistently (for example START and pediatric JumpSTART) and reassess categories as condition or resource availability changes.
- Use mass-casualty tag priorities to sequence care under scarcity (
REDimmediate life threat,YELLOWurgent major injury,GREENdelayed minor injury,BLACKexpectant/deceased). - Use an incident-command framework to assign clear responsibilities and improve coordination during rapidly evolving disaster response operations.
- Activate NIMS/ICS role structure early in MCI events to align interagency communication, resource tracking, and medical-branch triage-treatment-transport operations.
- Direct ambulatory casualties through contamination screening and decontamination pathways before unsupervised movement to reduce secondary spread risk.
- In CBRN-risk incidents, run zone-based operations: restrict hot-zone entry, perform decontamination/rapid triage in warm zone, and deliver treatment in cold zone.
- Activate surge-capacity plans by opening additional care areas, mobilizing supplemental staffing, and reallocating constrained resources.
- During infectious or mixed-hazard disasters, enforce containment operations with isolation precautions, PPE, environmental cleaning, and cohorting workflows.
- Provide psychological first-response actions: promote safety, calm, connectedness, self-efficacy, and practical hope.
- Initiate decontamination protocols when contamination indicators are present or when protocol criteria support precautionary decontamination.
- Use hazard-specific interventions (for example oxygenation support, antidote/chelation pathways, communicable-disease precautions, and mandatory reporting channels) according to presentation.
- During infectious outbreaks, support epidemiologic tracking, community screening/testing, vaccine operations, direct care delivery, and public prevention education.
- During biological-disaster response, escalate infection-prevention measures quickly (hand hygiene, PPE, isolation, and exposure follow-up) while coordinating with public-health reporting channels.
- For suspected biologic mass exposure, implement exposure-recognition workflow: restrict additional exposure, establish decontamination-treatment-clean zones, activate command chain, and triage/treat/transport casualties.
- During technological-disaster response, activate downtime communication/documentation plans, preserve medication/device safety controls, and isolate compromised systems per cyber-incident policy.
- Coordinate with public-health and emergency partners to request Strategic National Stockpile/medical countermeasure support when local critical assets are insufficient.
- During epidemic/pandemic response, reinforce triage-screening entry workflows, immediate isolation for suspected cases, and sustained community education on hygiene, vaccination, and early-care seeking.
- During high-fatality respiratory outbreaks, deploy nonpharmacologic control bundles early and monitor adherence consistency across sites.
- During outbreak communication, convert technical findings into plain-language actions, acknowledge uncertainty transparently, and repeat updates through trusted channels.
- Use non-stigmatizing language and equity-centered outreach in all pandemic messaging to prevent avoidable exclusion from testing, treatment, and follow-up care.
- Clarify team communication roles and spokesperson responsibilities early in response operations to reduce mixed messaging.
- Coordinate with local/state/federal emergency structures as surge thresholds exceed routine institutional capability.
- Build culturally inclusive preparedness plans by using multilingual messaging, accommodating culturally linked dietary or mourning practices in shelter workflows, and partnering with community leaders/organizations.
- Use ongoing continuing education and rapid evidence updates (for example PPE, transmission precautions, emerging therapeutics) to maintain safe response practice.
- Use pre-event nurse preparedness checklists that clarify alerts/warnings, employer role expectations, applicable state disaster obligations, travel-to-work contingencies, and family communication plans.
- Use organization-specific evacuation routes and shelter locations, and account for mobility-limited patients who cannot self-evacuate.
- Educate high-risk patients/families to maintain a ready emergency kit (essential medications, key documents, and basic supplies) for rapid displacement events.
- Support recovery with repeated behavioral health surveillance, community resource linkage, and resilience-focused education.
Secondary Contamination Risk
Delayed isolation or decontamination can harm responders, staff, and other patients while disrupting facility operations.
Pharmacology
Pharmacologic management in disasters is exposure-dependent and may include oxygen therapy, antidotes, chelating agents, antimicrobials, sedatives for severe agitation, or seizure-control agents. Medication strategy must align with triage priority and hazard-specific protocols.
Clinical Judgment Application
Clinical Scenario
After a chemical-release incident, several patients arrive simultaneously with respiratory symptoms, anxiety, and possible skin contamination.
- Recognize Cues: Multiple casualties, possible toxic exposure, and contamination risk to staff and environment.
- Analyze Cues: Immediate priorities are airway-breathing-circulation, contamination control, and triage categorization.
- Prioritize Hypotheses: Highest risk includes rapid respiratory decline and secondary contamination in the receiving area.
- Generate Solutions: Activate disaster protocol, assign triage categories, start decontamination pathway, and deploy behavioral support actions.
- Take Action: Implement PPE-protected intake, hazard-specific treatment, and coordinated reporting/escalation.
- Evaluate Outcomes: Casualty flow stabilizes, secondary exposure is prevented, and high-risk patients receive timely definitive care.
Related Concepts
- patient-admission-types-triage-and-room-readiness - Admission-level triage and throughput priorities during routine and surge operations.
- individual-and-environmental-safety-in-nursing-practice - Environmental hazard recognition and prevention-focused safety planning.
- safety-data-sheets-and-chemical-hazard-communication - Chemical hazard identification and exposure-response documentation.
- stress-crisis-staging-and-type-specific-nursing-response - Crisis and behavioral-response management in disaster-affected populations.
- Public Health Nursing - Community-level nursing coordination across prevention, emergency response, and recovery.
Self-Check
- Why does social-vulnerability mapping change disaster planning priorities?
- Which findings should trigger immediate decontamination precautions before routine intake?
- How does behavioral health surveillance change from response phase to recovery phase?