Maternal Substance Use sa Panahon ng Pagbubuntis
Mahahalagang Punto
- Ang substance use disorder sa pagbubuntis ay high-risk condition na kaugnay ng maternal at fetal morbidity at mortality.
- Inirerekomenda ang universal prenatal screening na may validated tools dahil karaniwan ang self-disclosure barriers.
- Nangangailangan ng follow-up assessment at intervention ang SURP positive screens (moderate/high risk).
- Nagbibigay ang SBIRT ng istrakturadong pathway: screening, brief motivational intervention, at referral to treatment.
- May legal at economic implications ang drug/alcohol testing; mahalaga ang informed consent, confirmatory testing, at state-law awareness.
- Dapat malinaw na isama sa pregnancy counseling ang nicotine/vaping, alcohol, marijuana, opioids, at iba pang illicit drugs dahil may magkakaibang maternal-fetal risks ang bawat isa.
- Pinapataas ng cocaine at methamphetamine use ang panganib ng migraine, seizure, prelabor rupture of membranes, at placental abruption.
Patopisyolohiya
Ang substance use disorder ay clinically significant pattern ng alcohol o drug use na nagpapagana ng reward pathways at nagpapahina sa judgment, self-care, at role function. Sa panahon ng pagbubuntis, pinapataas ng tuloy-tuloy na exposure ang panganib ng obstetric at neonatal complications, kabilang ang fetal alcohol spectrum disorder at neonatal abstinence syndrome.
Maaaring magpabagal sa disclosure at treatment entry ang behavioral at structural barriers (stigma, takot sa legal consequences, limitadong kaalaman sa treatment, at mababang tiwala sa care systems).
Klasipikasyon
- Low-risk screen: Walang affirmative SURP risk responses.
- Moderate-risk screen: Isang affirmative SURP item; nangangailangan ng karagdagang assessment.
- High-risk screen: Dalawa o tatlong affirmative SURP items; nangangailangan ng agarang follow-up at treatment linkage.
- Co-occurring risk context: Kasabay na mental-health disorders at IPV na nangangailangan ng integrated prenatal care planning.
Pagtatasa sa Pag-aalaga
Pokus sa NCLEX
Gumamit ng private, nonjudgmental, universal screening; huwag umasa lamang sa spontaneous disclosure.
- I-screen ang lahat ng buntis na kliyente gamit ang validated tools ayon sa protocol (halimbawa 4 P’s o SURP).
- Kapag available, gumamit ng validated tool options na tumutugma sa setting/workflow (halimbawa 4P’s, NIDA Quick Screen, CRAFFT, at SURP-context instruments).
- I-screen ang specific exposure categories: tobacco/vaping nicotine, alcohol, marijuana, opioids, at iba pang illicit substances, kabilang ang timing mula nang makilala ang pagbubuntis.
- Gamitin ang SURP question domains: marijuana history, alcohol use bago makilala ang pagbubuntis, at perceived need na magbawas.
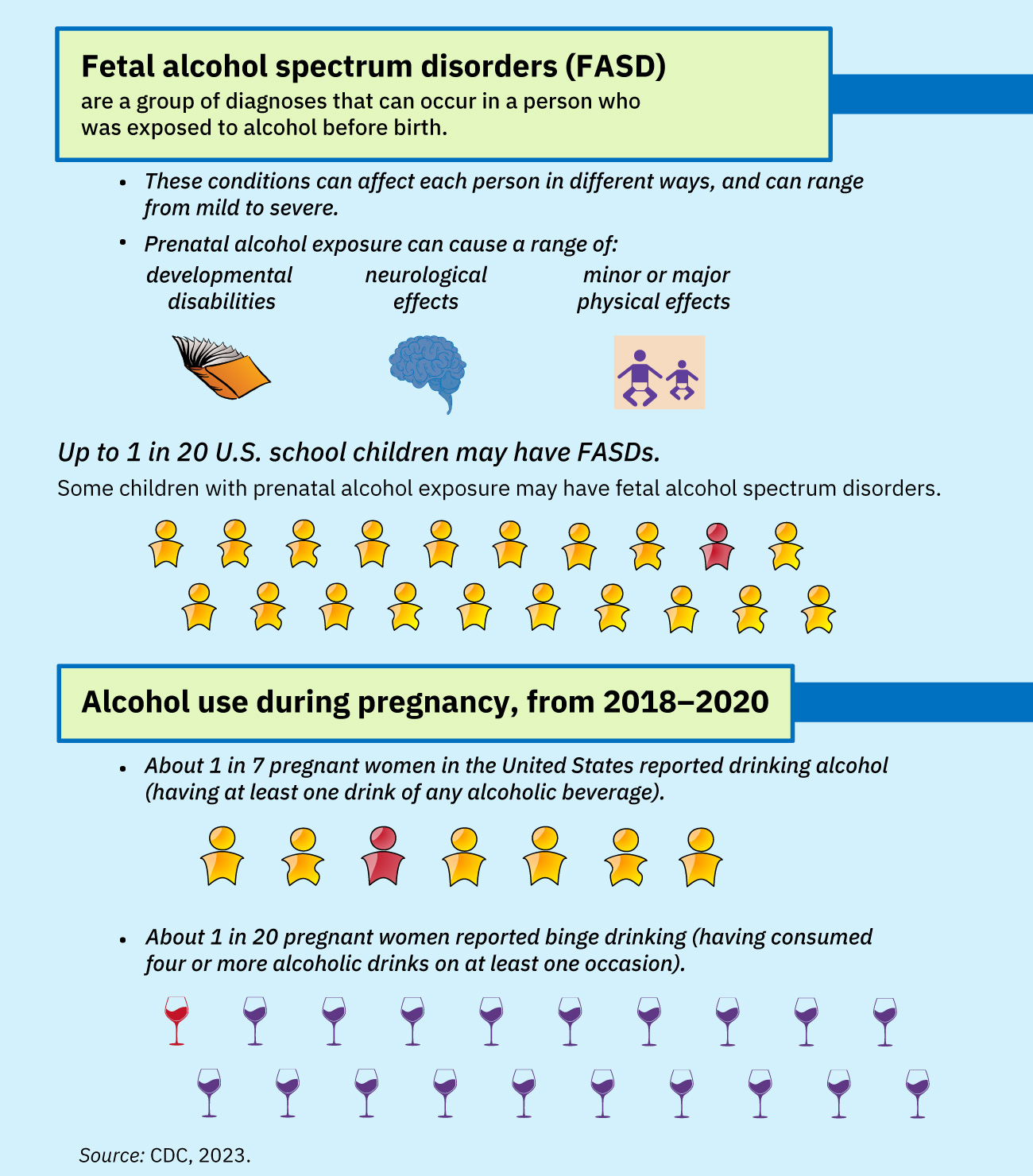 Illustration reference: OpenStax Clinical Nursing Skills Ch.20.2.
Illustration reference: OpenStax Clinical Nursing Skills Ch.20.2.
- I-classify ang screen results at idokumento ang objective risk level para sa follow-up planning.
- Tayahin ang barriers sa disclosure at treatment engagement (stigma, legal concerns, hopelessness, limitadong kaalaman).
- Tayahin ang karagdagang gendered barriers (halimbawa child-custody fear, caregiving-role pressure, at limitadong access sa women-focused treatment programs).
- Tayahin ang kasabay na depression, anxiety, trauma, at IPV dahil karaniwan ang overlap nito sa prenatal substance misuse.
- Kung isasaalang-alang ang laboratory testing, i-verify ang informed-consent requirements at state-specific testing/reporting rules.
- Kumpirmahing sinusundan ng confirmatory testing ang positive initial toxicology screens upang mabawasan ang false-positive harm.
- Sa panahon ng labor, tasahin ang posibleng acute intoxication at kaugnay na obstetric instability.
Mga Interbensiyong Pang‑nars
- Ipatupad ang SBIRT pagkatapos ng positive screening upang mapabuti ang insight at kahandaan para sa behavior change.
- Maghatid ng brief intervention gamit ang non-stigmatizing communication at motivational interviewing principles.
- Abisuhan ang provider sa positive screens at i-coordinate ang referral sa counseling, recovery services, at community resources.
- Magbigay ng patient education tungkol sa maternal-fetal risks at harm-reduction steps habang sinisimulan ang treatment (halimbawa low birth weight, preterm birth, placental abruption, fetal demise, neonatal withdrawal, SIDS, at neurodevelopmental effects).
- Sa opioid-use disorder, suportahan ang medication-for-opioid-use-disorder referral (halimbawa methadone o buprenorphine pathways) upang mabawasan ang relapse at unmanaged withdrawal risk.
- Palakasin ang postpartum newborn monitoring needs kapag may prenatal opioid o sedative exposure dahil maaaring lumitaw ang withdrawal pagkatapos ng kapanganakan.
- I-coordinate ang integrated care para sa co-occurring conditions (mental-health disorders, IPV, social instability).
- Ituro na dapat agad itigil ang stimulant use sa pagbubuntis at na contraindication sa breastfeeding ang patuloy na stimulant use.
- Kung nakuha ang toxicology ayon sa policy at positive sa delivery, abisuhan ang newborn care teams (nursery/NICU) para sa enhanced monitoring planning.
- Idokumento ang screening results, counseling content, consent status, at referral follow-through.
Legal and Reporting Harm Risk
Ang substance testing nang walang malinaw na consent/legal workflow ay maaaring lumikha ng maiiwasang legal, economic, at care-access harms.
Farmakolohiya
Ang medication decisions ay individualized ayon sa uri ng substance, withdrawal risk, gestational age, at treatment setting. Ang nursing priorities ay screening-identified escalation, safety monitoring, at linkage to treatment sa halip na unsupervised medication advice.
Aplikasyon ng Clinical Judgment
Klinikal na Sitwasyon
Isang prenatal na pasyente ang nag-screen na moderate-risk sa SURP at nag-uulat ng takot sa legal consequences kung maidadokumento ang substance use.
- Recognize Cues: Positive screening result kasama ang pangunahing disclosure barrier.
- Analyze Cues: Kung walang tiwala at istrakturadong follow-up, malamang ang treatment delay at mananatiling mataas ang maternal-fetal risk.
- Prioritize Hypotheses: Agarang prayoridad ang confidential, nonjudgmental engagement na may SBIRT at referral activation.
- Generate Solutions: Magbigay ng brief intervention, ipaliwanag ang consent/reporting framework, at simulan ang treatment-resource linkage.
- Take Action: I-coordinate ang provider notification, referral, at documented follow-up plan.
- Evaluate Outcomes: Nakikilahok ang pasyente sa tuloy-tuloy na care at recovery support na may nabawasang prenatal risk exposure.
Mga Kaugnay na Konsepto
- substance use disorders - Core SUD neurobiology at treatment framework na batayan ng prenatal risk.
- opioid use disorder - Mahahalagang subtype na may implikasyon sa pregnancy at neonatal abstinence.
- mga neonatal effect ng prenatal substance exposure - Newborn withdrawal at FASD-focused postbirth management priorities.
- domestic at intimate partner violence - Madalas kasabay ng prenatal substance-use risk ang IPV at dapat co-screened.
- mga psychosocial na aspekto ng pagbubuntis - Malakas ang impluwensiya ng social stress at stigma sa disclosure at treatment engagement.
Self-Check
- Aling SURP result patterns ang nangangailangan ng follow-up intervention?
- Bakit mas pinipili ang SBIRT kaysa one-time counseling pagkatapos ng positive prenatal substance screen?
- Bakit kritikal ang confirmatory tests at informed consent kapag nagsasagawa ng prenatal toxicology?