Family Dynamics, Stress, ACEs, at Multisystem Health Outcomes
Mahahalagang Punto
- Ang healthy family dynamics ay nagpapababa ng stress load at sumusuporta sa coping, sleep, at behavioral stability.
- Pinapataas ng dysfunctional dynamics at adverse childhood experiences ang risk para sa mental illness, substance use, at chronic disease.
- Hinuhubog ng family communication quality ang resilience, adherence, at recovery sa panahon ng acute at chronic illness.
- Maaaring putulin ng maagang pagkilala at family-level interventions ang intergenerational risk cycles.
- Dose-related ang ACE burden: kaugnay ng mas mataas na exposure ang mas maraming adolescent risk behaviors, mas mataas na adult chronic-disease burden, at mas maikling life expectancy.
- Karamihan ng adults ay nag-uulat ng kahit isang ACE, at ang apat o higit pang ACEs ay kaugnay ng mas mababang educational attainment at unemployment risk.
- Mataas ang U.S. adult ACE burden (humigit-kumulang 61% na may kahit isang ACE; 16% na may apat o higit pa), na may disproportionate four-or-more burden sa females at maraming racial/ethnic minority populations.
- Sa isang 2024 child-population meta-analysis, 15% ang may apat o higit pang ACEs, na mas mabigat ang burden sa residential-care, juvenile-offending, at Indigenous populations.
- Pinapabuti ng positive family dynamics ang sleep quality, stress regulation, at relationship resilience, lalo na sa adolescents.
- Maaaring magpahina ng family function ang illness (disequilibrium, conflict, role strain) ngunit maaari ring magpataas ng cohesion kapag malakas ang coping systems.
Patopisyolohiya
Ang family stress at relational instability ay nagpapagana ng chronic stress pathways, pinapataas ang allostatic burden, at nakaaapekto sa neuroendocrine, cardiovascular, metabolic, at behavioral outcomes. Maaaring baguhin ng paulit-ulit na adverse exposures sa childhood ang developmental trajectories at coping patterns.
Maaaring magsimula nang prenatal ang early biologic vulnerability. Ang maternal anxiety/depression burden at disrupted early attachment ay maaaring magbago ng infant cortisol patterning, na nagpapataas ng risk para sa kalaunang psychopathology kapag kulang ang protective supports.
Ang positive dynamics (secure attachment, constructive communication, consistent support) ay nagba-buffer ng stress physiology at nagpapabuti ng long-term outcomes. Ang negative dynamics (violence, neglect, chaos, isolation) ay nagpapalakas ng risk at nagpapalala ng disease management.
Klasipikasyon
- Protective dynamics: Cohesion, emotional responsiveness, adaptive communication, shared healthy habits.
- Risk dynamics: Conflict escalation, communication breakdown, neglect/abuse, instability, substance misuse.
- ACEs domains: Violence exposure, parental mental illness/substance use, housing/food insecurity, loss/separation, at traumatic caregiver relationships na nagbabago sa self-concept at future relationship patterns.
- Childhood stress-response continuum: Positive stress (maikling mild activation), tolerable stress (mas malaki ngunit time-limited activation na may buffer mula sa supportive adults), at toxic stress (madalas na prolonged adversity nang walang buffering support) kung saan ang toxic stress ang nagtutulak ng neurodevelopmental at long-term disease risk.
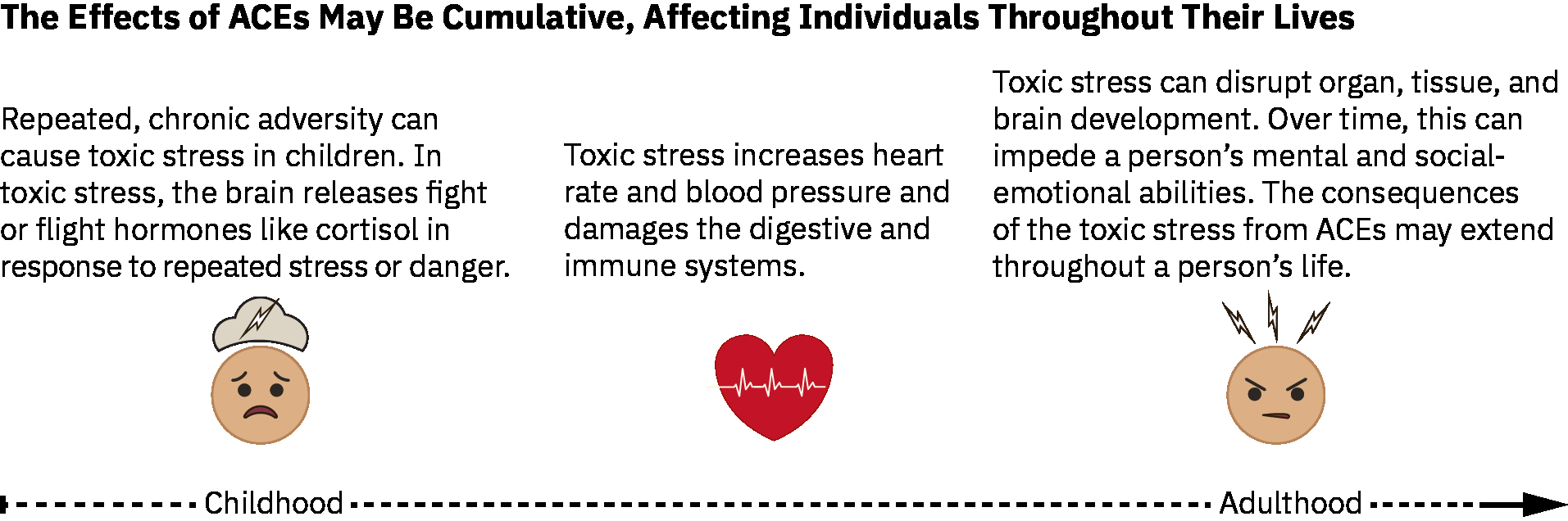 Illustration reference: OpenStax Population Health for Nurses Ch.27.6.
Illustration reference: OpenStax Population Health for Nurses Ch.27.6.
- Family risk-factor domains: Caregiver developmental/knowledge limitations, prior caregiver abuse history, financial strain, inconsistent discipline, low supervision, social isolation, at high interpersonal conflict.
- Family-system stressor framework: Demands, control, support, relationships, role clarity, at major change events.
- Community risk-factor domains: Violence/crime burden, poverty/unemployment, food insecurity, unstable housing, substance availability, at mababang youth/community engagement.
- Protective-factor domains: Stable nurturing relationships, basic-needs security, supportive mentor access, positive parenting, school engagement, at community childcare/after-school supports.
- Outcome domains: Anxiety/depression, addiction risk, sleep disturbance, cardiometabolic at functional decline.
- Extended ACE outcome domain: Kaugnay ng mas mataas na ACE burden ang risky sexual behavior at pagtaas ng long-term malignancy/cardiovascular/metabolic disease risk.
- Pediatric burden anchor: Sa isang pediatric population comparison, ang mga batang may 3 o higit pang iniulat na ACEs ay may kapansin-pansing mas mataas na prevalence ng mental/emotional/behavioral disorders kumpara sa may 0 ACEs (36.3% vs 11.0%).
- Pediatric prevalence distribution anchor: Sa isang 2024 meta-analysis sa child populations, ang ACE prevalence ay humigit-kumulang 42% (0 ACE), 22% (1 ACE), 13% (2 ACEs), 8% (3 ACEs), at 15% (4 o higit pang ACEs), na may mas mataas na 4+ burden sa residential-care, juvenile-offending, at Indigenous groups.
- Positive-outcome domains: Mas mabuting sleep quality/duration, mas mababang stress burden, mas matatag na interpersonal conflict resolution, at pinahusay na illness recovery.
- Negative-disease-burden domains: Depression, anxiety, addiction, atherosclerotic/cardiometabolic risk, asthma/ulcer burden, at mas malawak na chronic-disease amplification sa ilalim ng persistent dysfunctional dynamics.
- Coping-style domains: Meaning-focused, problem-focused, at emotion-regulation-focused patterns na may mixed-strategy use bilang karaniwang real-world pattern.
Nursing Assessment
Pokus sa NCLEX
Suriin ang family stressors bilang clinical risk factors, hindi bilang background social details.
- Suriin ang family communication patterns at coping style sa ilalim ng stress.
- Suriin ang kasalukuyang family stressor load gamit ang common triggers (halimbawa housing change, role confusion, death/divorce, financial strain, overloaded schedules, serious illness, at work-life imbalance).
- Suriin ang ACE-related exposures at kasalukuyang safety concerns.
- Suriin ang health-behavior patterns (sleep, activity, diet, substance use) na hinuhubog ng family context.
- Suriin ang role strain at caregiver burden sa panahon ng illness-related role shifts.
- Suriin ang child/adolescent risk behaviors at chronic-risk trajectory kapag mataas ang ACE burden.
- Suriin ang family at community protective assets na maaaring agad i-mobilize (mentors, school supports, childcare, housing, at financial resources).
- Suriin ang transition-phase stress sa launching/senior life-cycle periods (halimbawa empty-nest grief, role/livelihood changes, intergenerational dependence shifts).
- Suriin ang maladaptive coping cues (halimbawa avoidance/isolation, relationship sabotage, substance misuse, o high-risk dopamine-seeking behaviors).
- Suriin ang nakikitang family-level stress reactions tulad ng tumitinding arguments, withdrawal/disconnection, overuse ng food/alcohol/substances, at kabiguang matugunan ang essential role duties.
- Suriin ang illness-phase burden sa family functioning, kabilang ang malamang na role reversal, “sick role” consolidation, at resentment risk kapag hindi hayagang napag-usapan ang role changes.
Nursing Interventions
- Gumamit ng trauma-informed at nonjudgmental communication upang mailabas ang mga nakatagong stressors.
- Magpatupad ng family-level coaching para sa sleep hygiene, stress regulation, at conflict de-escalation.
- Iugnay nang maaga ang families sa counseling, social work, at community resources.
- Suportahan ang early caregiver-infant bonding at perinatal mental-health referral kapag mataas ang prenatal o postnatal stress burden.
- Palakasin ang protective routines at strengths upang bumuo ng sustainable resilience.
- Ituro nang hayagan ang coping-strategy selection (meaning-focused vs problem-focused vs emotion-focused) at i-normalize ang paggamit ng kombinasyon sa paglipas ng panahon.
- Suportahan ang ACE prevention sa pamamagitan ng parent education, consistent supervision/discipline coaching, at linkage sa economic, housing, at mental-health resources.
- Gamitin ang CDC ACE-prevention framework kapag nagpaplano ng community actions: palakasin ang economic family supports, itaguyod ang nonviolence social norms, tiyakin ang strong start para sa children, ituro ang coping/relationship skills, iugnay ang youth sa caring adults at activities, at maagang mag-intervene upang mabawasan ang short- at long-term harm.
- Isama ang population-prevention pathways kapag available: economic family supports, high-quality childcare/preschool, healthy-relationship education, at youth-to-caring-adult connection programs.
- Makipagtulungan sa community pathways (halimbawa after-school programs at safe childcare/preschool supports) upang mabawasan ang ongoing exposure risk.
- I-normalize ang help-seeking para sa parenting stress, substance misuse, depression, at suicidal thoughts upang mabawasan ang ACE-related stigma barriers.
- Sa routine encounters, tukuyin nang maaga ang ACE risk cues at i-refer ang youth/families sa evidence-based prevention at support services.
- Sa illness-triggered role shifts, padaliin ang structured role renegotiation upang maiwasan ang unsafe burden concentration at unresolved resentment.
- Ilapat ang primary ACE prevention sa pamamagitan ng upstream advocacy at linkage (halimbawa affordable housing, living-wage/economic supports, food assistance, parenting support, at violence-prevention resources).
- Ilapat ang secondary prevention sa pamamagitan ng pagtukoy sa ACE exposure risk, pagsusuri ng protective factors, at paggamit ng standardized ACE-informed screening workflows lamang kapag may available na referral/treatment pathways.
- Ilapat ang tertiary prevention sa pamamagitan ng pagbawas ng downstream harm gamit ang trauma-focused counseling referral, social-support network building, at stress-regulation teaching (halimbawa paced breathing at meditation).
Intergenerational Risk Reinforcement
Ang hindi natutugunang ACE-related dynamics ay maaaring magpatuloy ng disease risk at dysfunction sa iba’t ibang henerasyon.
Pharmacology
Mas epektibo ang medication plans kapag kasabay na tinutugunan ang family stressors at adherence barriers kasama ng symptom treatment.
Clinical Judgment Application
Clinical Scenario
Isang family na may paulit-ulit na emergency visits ang may mahinang tulog, mataas na conflict, caregiver exhaustion, at adolescent substance use.
- Recognize Cues: Multi-domain stress pattern na may posibleng ACE carryover.
- Analyze Cues: Ang family dynamics ang nagtutulak ng recurrent health instability.
- Prioritize Hypotheses: Agarang prayoridad ang safety, stabilization, at coping infrastructure.
- Generate Solutions: Magpatupad ng family-centered counseling/referral at behavior-reset plan.
- Take Action: I-coordinate ang interprofessional support at i-monitor ang adherence/response.
- Evaluate Outcomes: Nabawasang crises, pinahusay na function, at mas malusog na family routines.
Mga Kaugnay na Konsepto
- stress response, homeostasis, at allostasis - Mechanistic stress model na pinagbabatayan ng family-dynamics effects.
- chronic stress, allostatic load, at system breakdown - Long-term disease burden mula sa unresolved stress.
- pagtingin sa family structure at mga implikasyon sa kalusugan - Structural context na humuhubog sa dynamic patterns.
- trauma-informed care - Core approach para sa ACE-related assessment at intervention.
- mga substance-use disorder - Karaniwang downstream manifestation ng maladaptive coping environments.
Sariling Pagsusuri
- Aling family-dynamics cues ang dapat mag-trigger ng maagang prevention-focused intervention?
- Paano nag-aambag ang ACEs sa kalaunang cardiometabolic at mental-health risk?
- Bakit madalas kinakailangan ang family-level interventions para sa matibay na individual outcomes?