Sputum Nasal and Oropharyngeal Specimen Collection
Key Points
- Specimen quality depends on collecting the right specimen material (true sputum, not saliva).
- Correct swab-site technique improves diagnostic yield for respiratory pathogens.
- Early-morning sputum collection and contamination control steps increase reliability.
- Sputum testing may be ordered for cytology, culture/sensitivity, or AFB evaluation; collection timing should match ordered test goals.
- PPE, labeling, and immediate transport are core safety and reliability controls.
- Respiratory-swab workflows require strict PPE use for collectors and nearby staff per policy.
Equipment
- Sterile sputum container
- Swab kit(s) for nasal, nasopharyngeal, or oropharyngeal collection
- Tongue depressor and penlight/flashlight for oropharyngeal visualization
- PPE appropriate to suspected pathogen/isolation level
- Biohazard transport bags, labels, and requisition materials
Procedure Steps
- Verify order, specimen type/site, and patient identity, including whether testing target is cytology, culture/sensitivity, or AFB/TB workflow.
- Complete hand hygiene, apply PPE based on isolation/pathogen risk (including respirator-level mask when required and eye/gown/glove protection for collectors and nearby staff per policy), and explain sensations expected during collection.
- Before sputum collection, optimize secretion mobilization:
- Encourage hydration when not contraindicated.
- Give ordered nebulizer treatment before collection when available.
- Address cough-limiting pain (for example after chest or abdominal surgery); consider splinting with a pillow.
- For culture/sensitivity workflows, collect before first antibiotic dose when clinically feasible because antimicrobial exposure can reduce organism recovery.
- Prefer early-morning sputum collection. Have the patient rinse with water only, avoid toothpaste/mouthwash, and remove dentures if present.
- Position patient upright (chair, bedside sitting, or High Fowler).
- Instruct three slow deep breaths followed by a deep cough; repeat with short rest periods until sputum is produced.
- Collect sputum directly into sterile container without touching inside surfaces. Target at least 5 mL (about 1 teaspoon).
- Confirm specimen quality: sputum is typically thick/opaque, while saliva is thin/clear/watery.
- Cap container tightly, label at bedside with patient identifiers and collection time, place in biohazard transport bag, and send promptly to the lab.
- For AFB/TB workflows, follow ordered serial collection pattern (commonly at least three consecutive sputum specimens, including at least one early-morning sample).
- If sputum cannot be expectorated, escalate supportive measures (hydration, nebulizer, deep breathing, chest percussion, postural drainage) and collaborate with respiratory therapy; suction-based collection may be required in intubated patients.
- For upper-airway swabs, use site-specific technique:
- Anterior nasal swab: tilt head back (commonly about 70 degrees), insert shallowly (commonly no more than about 0.5 in/1.25 cm), leave in place about 10 to 15 seconds, then repeat in the opposite nostril.
- Nasopharyngeal swab: ask the patient to tilt the head slightly back, insert through one nostril posteriorly along natural curvature, and advance approximately ear-to-nostril distance; if resistance occurs, adjust angle or use the other nostril, and do not force insertion. Once the nasopharynx is reached, rotate for several seconds, then withdraw slowly while continuing to rotate.
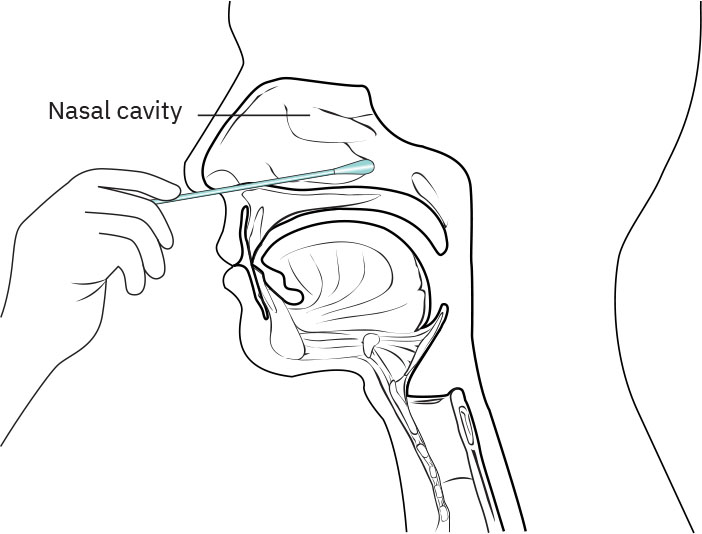 Illustration reference: OpenStax Clinical Nursing Skills Ch.10.
Illustration reference: OpenStax Clinical Nursing Skills Ch.10. - Swab tube handling: place swab in sterile collection tube per manufacturer instructions, usually swab-first with break-off at etched groove before capping.
- Oropharyngeal swab: direct swab to posterior throat while patient says “ahh”; avoid tongue, teeth, and gums; collect from ordered target area (tonsils alone or posterior pharynx plus tonsillar area), including bilateral tonsillar pillars when ordered. Use a tongue depressor and penlight as needed for visualization, and coach that brief gag/discomfort can occur.
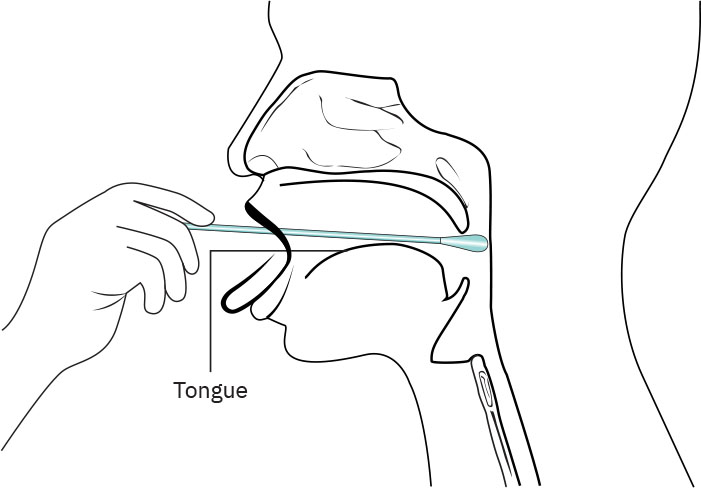 Illustration reference: OpenStax Clinical Nursing Skills Ch.10.
Illustration reference: OpenStax Clinical Nursing Skills Ch.10. - If gagging interrupts collection, pause and allow rest, then reattempt with coaching strategies (for example focusing gaze on the ceiling or closing eyes) while preserving target-area access.
- Pediatric support: infants/children may require a second trained assistant or parent-supported stabilization to keep the head/mouth still and reduce nasal/nasopharyngeal/oropharyngeal injury risk; explain expected positioning and roles before collection.
- Label specimen tube at bedside with required identifiers per policy (commonly name, DOB, medical-record number, collection date/time, collector initials, and specimen type), then place in biohazard transport bag.
- Document specimen type, collection date/time, specimen quality and appearance (including amount/color for sputum), recent antibiotic therapy, oral/nasal structure appearance, patient tolerance, unexpected outcomes/interventions, and teaching given with comprehension/follow-up needs.
Common Errors
- Submitting saliva instead of sputum → low diagnostic value.
- Incorrect swab-site depth/path → false-negative risk.
- Delayed transport or unlabeled specimen → unreliable or rejected results.
Related
- sputum-culture-and-acid-fast-testing-for-tuberculosis - Diagnostic rationale and TB-focused serial sampling principles.
- standard-precautions - Core infection-control framework during specimen handling.
- culture-and-sensitivity-testing-in-infection-management - Specimen quality affects targeted antimicrobial planning.
Patient Education Highlights
- Explain why sputum or upper-airway specimen collection is needed.
- Teach ideal collection timing (often morning for sputum) and preparation steps.
- Reinforce no food or drink for at least 30 minutes before sputum collection when ordered to reduce saliva contamination.
- Reinforce hand hygiene before specimen handling and correct container use.
- Coach effective cough technique and emphasize avoiding saliva contamination.
- Explain when and how results will be communicated and when to seek follow-up.
- If infectious symptoms are present, reinforce respiratory hygiene.
- For nasal/oropharyngeal swabs, prepare patients for possible brief gag reflex or discomfort; coach them to remain still, avoid pulling away, and breathe through the nose.