Fetal Alcohol Spectrum Disorders
Key Points
- FASD encompasses a spectrum of disorders caused by prenatal alcohol exposure (PAE), from mild neurobehavioral deficits to full fetal alcohol syndrome.
- FAS is the most severe form, featuring characteristic facial dysmorphisms (smooth philtrum, thin upper lip, small palpebral fissures), growth deficits, and CNS abnormalities.
- No amount of alcohol during pregnancy is considered safe; FASD is preventable.
- FASD requires lifelong multidisciplinary support; early intervention improves outcomes.
Pathophysiology
Alcohol consumed during pregnancy crosses the placenta and reaches the fetus, which metabolizes alcohol more slowly than the adult. Alcohol disrupts fetal development through multiple mechanisms: direct teratogenic effects on developing tissues, interference with oxygen delivery and nutritional intake, and epigenetic alterations affecting gene expression. The severity of FASD depends on genetic susceptibility, timing of exposure relative to developmental stage, drinking pattern, and amount consumed. Prevalence ranges from 3 to 5 percent in Europe and North America.
FASD Classifications
- Fetal alcohol syndrome (FAS): The most severe form; includes three facial abnormalities, growth deficit, and CNS abnormalities.
- Partial FAS: Some but not all hallmark features of FAS.
- Alcohol-related neurodevelopmental disorder: Intellectual disabilities or behavioral/learning problems without full facial features.
- Alcohol-related birth defects: Congenital and genetic birth defects from PAE.
- Neurobehavioral disorder associated with PAE: Neurocognitive impairments including memory, impulse control, and daily living difficulties.
Clinical Manifestations
- Facial features (FAS): Smooth philtrum, thin upper lip (vermilion border), small palpebral fissures.
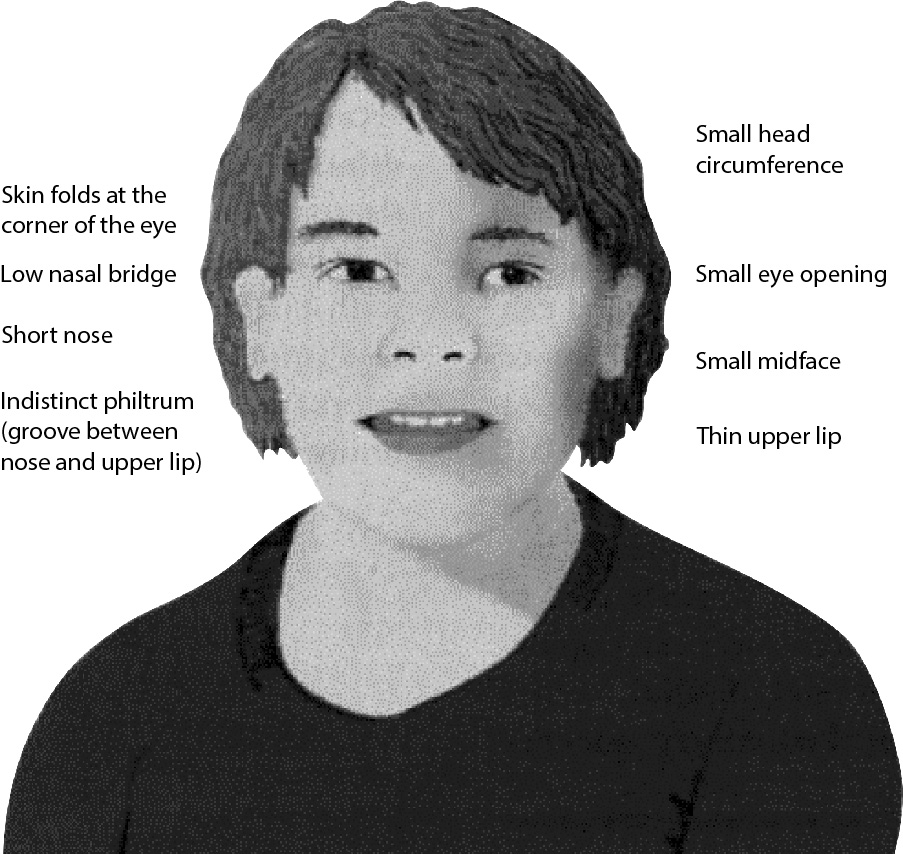 Illustration reference: OpenStax Clinical Nursing Skills Ch.26.3.
Illustration reference: OpenStax Clinical Nursing Skills Ch.26.3.
- Growth: Below-average height and/or weight (prenatal and postnatal growth restriction).
- CNS: Microcephaly, intellectual disability, learning difficulties, poor coordination, behavioral problems.
- Behavioral: Poor impulse control, hyperactivity, difficulty with social interactions, vulnerability to mental health disorders.
Nursing Assessment
- Assess for characteristic facial dysmorphisms at birth and during early childhood.
- Evaluate growth parameters (head circumference, length, weight) against expected norms.
- Obtain a thorough maternal history including alcohol use during pregnancy (nonjudgmental, open-ended questioning).
- Screen for neurodevelopmental delays using age-appropriate developmental tools.
- Assess for overstimulation in neonates with FAS (agitation, difficulty self-soothing).
- Evaluate family support systems and need for social services.
Nursing Interventions
- Provide a calm, low-stimulation environment for neonates with FAS; cluster care to minimize disruption.
- Coordinate early intervention services: speech therapy, physical therapy, occupational therapy.
- Educate the birthing person that no amount of alcohol during pregnancy is safe.
- Refer for alcohol cessation programs and support groups if substance use is ongoing.
- Connect families with social services, early intervention programs, and support resources.
- Assess siblings for potential FASD if maternal alcohol use occurred during other pregnancies.
- Provide genetic counseling referral when appropriate.
Related Concepts
- neonatal-bonding-feeding-and-newborn-screening - Early identification of congenital anomalies.
- substance-use-disorders - Maternal alcohol use and intervention strategies.
- Developmental Milestones - Monitoring neurodevelopmental progress.
- Prenatal Care - Prevention through alcohol avoidance education.
- Coping And Stress Tolerance - Family support for lifelong disability management.
Self-Check
- What are the three characteristic facial features of fetal alcohol syndrome?
- Why does the fetus experience higher concentrations of alcohol than the mother?
- What is the single most effective prevention strategy for FASD?