Endometriosis
Key Points
- Endometriosis involves endometrial-like tissue growth outside the uterus with chronic inflammation and scarring.
- Common implant locations include ovaries, fallopian tubes, peritoneum, bladder, and bowel-related pelvic surfaces.
- Symptom expression is variable; some patients are minimally symptomatic or asymptomatic despite significant disease.
- Onset can occur from early reproductive years and may persist until menopause.
- Etiology is multifactorial and not fully established, with proposed contributions from retrograde flow, genetic factors, and hormonal/immune dysregulation.
- There is no definitive cure; treatment focuses on pain control, function, and fertility-centered planning.
Pathophysiology
Endometriosis is characterized by ectopic endometrial-like tissue outside the uterine cavity. Cyclic activity of these lesions contributes to persistent inflammatory signaling, fibrosis, and scar-tissue formation in pelvic structures.
Potential disease mechanisms include retrograde menstrual flow, genetic predisposition, and hormonal or immune-system abnormalities. No single mechanism fully explains all presentations. In U.S. persons AFAB, prevalence is commonly reported near one in ten, with diagnosis often delayed by symptom variability and overlap with other pelvic pain conditions.
Classification
- Pelvic-peritoneal pattern: Implants on peritoneal surfaces and adjacent pelvic organs.
- Ovarian involvement pattern: Ovarian implant burden with inflammatory pain and reproductive impact.
- Deep infiltrative pattern: Lesions extending into surrounding structures such as bowel or bladder interfaces.
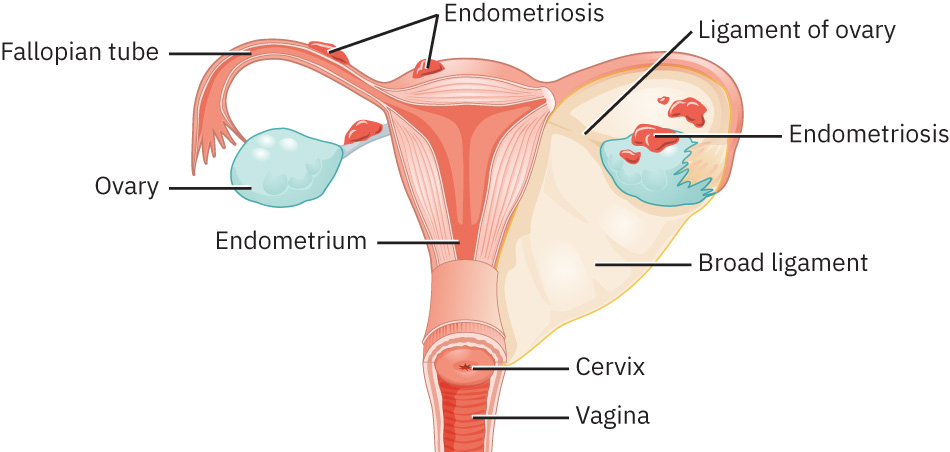 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.1.
Nursing Assessment
NCLEX Focus
Prioritize chronic cyclic pelvic-pain patterns and assess functional burden over time.
- Assess pain trajectory across cycles and daily function impact.
- Screen for high-yield symptoms: chronic pelvic pain, dysmenorrhea, heavy menstrual bleeding, dyspareunia, and infertility concerns.
- Include intermenstrual spotting and pain during or after sex in symptom-pattern review.
- If bowel or bladder involvement is suspected, assess GI/urinary features such as painful bowel movements during menses, bloating/constipation/diarrhea, or dysuria.
- Assess reproductive goals and concerns early because fertility impact is common.
- Document prior evaluations and treatment responses to guide escalation planning.
- Reinforce diagnostic pathway expectations: ultrasound/MRI can support evaluation, but laparoscopic direct visualization with biopsy remains definitive.
Nursing Interventions
- Provide disease education focused on chronic inflammatory nature and individualized long-term management.
- Teach multimodal treatment goals: pain control, quality-of-life improvement, and fertility planning.
- Reinforce that treatment can begin from clinical suspicion and imaging findings even when definitive laparoscopy has not yet been performed.
- Support symptom tracking tools to improve follow-up decisions.
- Reinforce referral/follow-up adherence with gynecology and fertility specialists when indicated.
- Provide ongoing emotional support and coping-resource linkage for chronic pain burden.
- Discuss that symptoms may improve around menopause as estrogen decline reduces endometrial activity.
- For severe or refractory disease, prepare patients for surgical options such as laparoscopic excision to reduce symptom burden and support fertility goals when appropriate.
- When patients use complementary approaches (for example acupuncture or supplements), reinforce shared decision-making and safety review with the care team.
Delayed-Diagnosis Risk
Recurrent pelvic pain and related symptoms should not be minimized; delayed recognition increases quality-of-life and fertility burden.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| nsaids | Ibuprofen, naproxen | Common first-line pain-control options while definitive diagnosis and longer-term planning proceed. |
| hormonal-therapy | Combined hormonal and progestin-based pathways | Used to suppress cyclical lesion activity and reduce pain burden in selected patients. |
| gonadotropin-releasing-hormone-gnrh-analogs (gnrh-analogs) | Leuprolide and related agents | Consider in persistent symptoms; monitor for adverse effects and follow-up adherence. |
Clinical Judgment Application
Clinical Scenario
A patient reports years of recurrent pelvic pain that intensifies around menstruation and now affects work attendance and relationships.
- Recognize Cues: Chronic cyclic pain pattern with growing functional impairment.
- Analyze Cues: Inflammatory pelvic disorder such as endometriosis is a high-priority differential.
- Prioritize Hypotheses: Confirm etiology while reducing pain burden and preserving fertility options.
- Generate Solutions: Coordinate targeted imaging/workup and initiate symptom-directed management plan.
- Take Action: Implement structured follow-up, medication education, and psychosocial support.
- Evaluate Outcomes: Symptoms become more controlled and the patient engages in longitudinal care planning.
Related Concepts
- dysmenorrhea - Endometriosis is a common cause of secondary dysmenorrhea.
- functional-reproductive-disorders - Endometriosis is a core inflammatory functional disorder in reproductive care.
- causes-of-infertility - Endometriosis may impair fertility through inflammatory and adhesive pathways.
- chronic-pelvic-pain - Persistent pelvic pain often overlaps with endometriosis presentations.
Self-Check
- Which pathophysiologic features distinguish endometriosis from simple primary menstrual pain?
- Why can endometriosis remain underdiagnosed for long periods?
- Which nursing assessments best capture functional burden in chronic endometriosis?