Personality Disorder Clusters A, B, and C
Key Points
- Personality disorders are organized into cluster A (odd/eccentric), cluster B (dramatic/erratic), and cluster C (anxious/fearful) patterns.
- Cluster A includes paranoid, schizoid, and schizotypal presentations marked by social detachment or unusual cognition.
- Cluster B includes antisocial, borderline, histrionic, and narcissistic presentations with impulsivity, emotional reactivity, and relational instability.
- Cluster C includes avoidant and dependent patterns characterized by fear, insecurity, and reliance on reassurance.
- Many personality-disorder patterns are ego-syntonic, so clients may not identify their behavior as problematic despite major functional harm.
Pathophysiology
Cluster expression reflects different mixtures of temperament, developmental adversity, cognitive schema formation, and relational-learning patterns. While all clusters show personality rigidity and impairment, each cluster expresses distinct affective and interpersonal organization.
Cluster A commonly emphasizes suspiciousness, interpersonal distance, or eccentric processing. Cluster B commonly emphasizes affective volatility, impulsivity, and identity/interpersonal instability. Cluster C commonly emphasizes fear-driven avoidance, dependence, or high reassurance-seeking.
Classification
- Cluster A (odd/eccentric): Paranoid, schizoid, schizotypal personality disorders.
- Cluster B (dramatic/emotional/erratic): Antisocial, borderline, histrionic, narcissistic personality disorders.
- Cluster C (anxious/fearful): Avoidant and dependent personality disorders.
Cluster A Diagnostic Anchors
- Paranoid personality disorder: Pervasive distrust and suspicious interpretation of others’ motives; DSM-5-TR diagnosis requires four or more persistent features (for example unjustified doubt about loyalty, hidden-threat interpretation of benign events, grudge-holding, or recurrent unjustified jealousy).
- Schizoid personality disorder: Detachment from social relationships with restricted emotional expression; DSM-5-TR diagnosis requires four or more persistent features (for example preference for solitary activities, little desire for close relationships, limited pleasure, indifference to praise/criticism, and emotional coldness or flat affect).
- Schizotypal personality disorder: Social/interpersonal deficits plus cognitive-perceptual distortions and eccentric behavior; DSM-5-TR diagnosis requires five or more features (for example ideas of reference, magical thinking, unusual perceptual experiences, odd speech/appearance, paranoid ideation, and persistent social anxiety linked to paranoid fears).
- Schizoid vs schizotypal distinction: Schizoid pattern centers on detachment and flat affect without cognitive-perceptual distortion, whereas schizotypal pattern includes eccentric cognition/perception in addition to social deficits.
Cluster B Diagnostic Anchors
- Antisocial personality disorder: Persistent disregard for and violation of others’ rights since age 15; DSM-5-TR diagnosis requires three or more features such as unlawful behavior, deceitfulness, impulsivity, aggressiveness, reckless disregard for safety, irresponsibility, and lack of remorse.
- Borderline personality disorder: Instability of relationships, self-image, and affect with marked impulsivity; DSM-5-TR diagnosis requires five or more features such as abandonment fear, splitting, identity disturbance, self-damaging impulsivity, recurrent suicidal or self-injurious behavior, affective lability, intense anger, and stress-related dissociation/paranoid ideation.
- Histrionic personality disorder: Excessive emotionality and attention-seeking; DSM-5-TR diagnosis requires five or more features such as discomfort when not center of attention, inappropriate seductive behavior, shallow/rapidly shifting emotion, impressionistic speech, theatrical expression, suggestibility, and overestimation of relationship intimacy.
- Narcissistic personality disorder: Grandiosity, need for admiration, and limited empathy; DSM-5-TR diagnosis requires five or more features such as exaggerated self-importance, fantasies of unlimited success/power, entitlement, exploitative behavior, lack of empathy, envy, and arrogant or haughty attitudes.
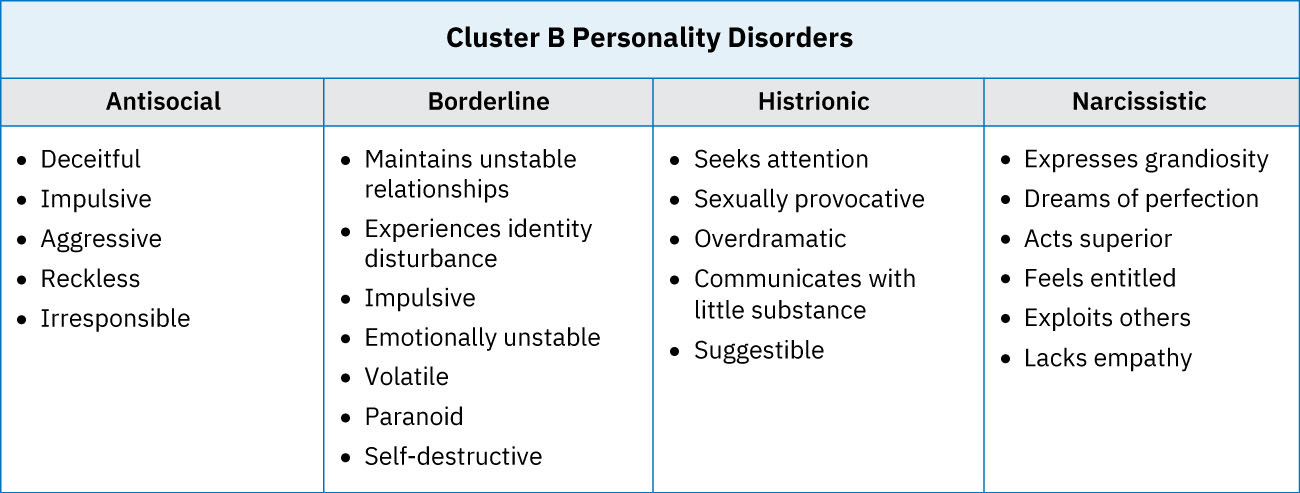 Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.18.2.
Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.18.2.
Cluster C Diagnostic Anchors
- Avoidant personality disorder: Social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation; DSM-5-TR diagnosis requires four or more features such as avoidance of interpersonal work situations, reluctance to engage unless certain of acceptance, fear of criticism/rejection, self-perceived inferiority, and risk-avoidant behavior due to embarrassment fears.
- Dependent personality disorder: Excessive need to be cared for with submissive/clinging behavior and separation fears; DSM-5-TR diagnosis requires five or more features such as reassurance-dependent decision-making, difficulty expressing disagreement, inability to initiate independently, urgent relationship-seeking after loss, and marked fear of being unable to care for self.
- Obsessive-compulsive personality disorder (OCPD): Pervasive perfectionism, orderliness, and control at the expense of flexibility/efficiency; DSM-5-TR diagnosis requires four or more features such as rigid rule focus, perfectionism that delays completion, overwork, reluctance to delegate, hoarding of worthless items, and stubbornness.
- OCPD vs OCD distinction: OCPD reflects enduring personality traits that are often ego-syntonic, whereas obsessive-compulsive disorder involves distressing obsessions/compulsions that are typically experienced as intrusive.
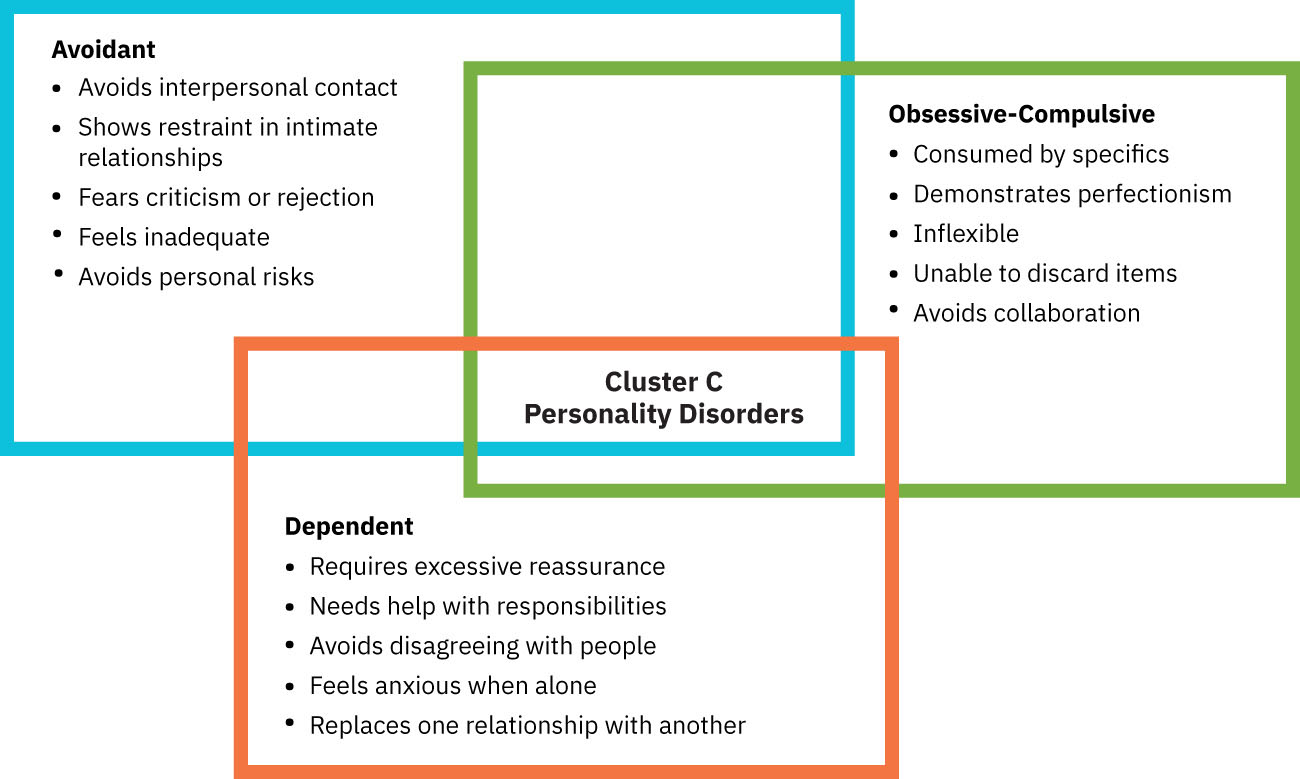 Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.18.2.
Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.18.2.
Nursing Assessment
NCLEX Focus
Identify cluster-level pattern first, then assess diagnosis-specific safety and functional risks.
- Assess baseline interpersonal style (detached, chaotic, or fear-dependent).
- Assess affective regulation, impulsivity, aggression risk, and self-harm risk.
- Assess social/occupational impairment and chronic relationship disruptions.
- Assess level of insight and treatment readiness, including resistance patterns.
- Assess co-occurring anxiety, mood symptoms, substance use, and trauma history.
Nursing Interventions
- Adapt communication style to cluster pattern while maintaining consistency and respect.
- Set clear limits and boundaries early, especially in high-manipulation or crisis-prone dynamics.
- Reinforce adaptive coping, emotional regulation, and interpersonal effectiveness skills.
- Use collaborative problem-solving to reduce splitting, avoidance, and treatment disengagement.
- Coordinate cluster-appropriate psychotherapy pathways and continuity planning.
Label-Driven Bias
Diagnostic labels can trigger staff bias; care quality improves when behavior is interpreted clinically, not morally.
Pharmacology
Medications are symptom-targeted rather than cluster-curative. Antidepressants, mood stabilizers, antipsychotics, and selected anxiolytics may be used for comorbid or severe symptom domains depending on presentation. Nurses monitor effectiveness, side effects, and behavioral change in context of psychotherapy goals.
Clinical Judgment Application
Clinical Scenario
A client shows intense relationship swings, impulsive conflict behavior, and recurrent emotional crises with episodic self-harm threats.
- Recognize Cues: Dramatic, unstable interpersonal and affective pattern.
- Analyze Cues: Cluster B features predominate with immediate safety implications.
- Prioritize Hypotheses: Priority is suicide/self-harm prevention and structured boundary-based care.
- Generate Solutions: Implement crisis plan, skills coaching, and psychotherapy engagement strategy.
- Take Action: Apply team-consistent limits, de-escalation, and close risk reassessment.
- Evaluate Outcomes: Track crisis frequency, interpersonal stability, and treatment adherence.
Related Concepts
- personality-disorder-identification-and-diagnosis - Defines diagnostic thresholds and assessment foundations.
- personality-disorder-nursing-care-and-treatment-approaches - Expands treatment modalities and nursing care plans.
- dissociative-identity-disorder - Supports differential assessment in complex identity and trauma presentations.
- anxiety-related-disorders - Helps separate anxiety-spectrum symptoms from cluster C personality pathology.
- client-engagement - Improves alliance and sustained participation in long-term care.