Mental Health in the Homeless and Displaced Population
Key Points
- Housing instability is both a cause and consequence of mental illness and substance-use disorders.
- Barriers include poverty, discrimination, legal entanglement, limited services, and psychosocial trauma burden.
- Recovery-oriented approaches require coordinated housing, health, behavioral health, and social support systems.
- Nurses are critical connectors for assessment, referral, advocacy, and cross-sector collaboration.
- Homelessness and health are bidirectional: health problems can lead to homelessness, homelessness can cause illness, and homelessness can block effective treatment.
- Low-threshold integrated medical-home models can reduce emergency visits and hospitalizations in unhoused populations.
- Person-centered terminology (for example unhoused/houseless preferences) and nonstigmatizing communication improve trust and engagement.
- Veterans, families with children, and rural communities require tailored outreach because barrier patterns and local resources differ.
- Community-based nursing encounters often pair mental-health support with practical frontline care (for example wound care, immunizations, and basic screening) to stabilize engagement.
- Point-in-time estimates in this source context highlight substantial unsheltered burden, requiring low-barrier outreach rather than clinic-only follow-up plans.
- In displaced populations, legal status differences (refugee vs asylum seeker) can alter resettlement pathways and practical access to health services.
- Refugee-care planning should integrate trauma-informed mental-health assessment with communicable-disease screening, vaccination review, and language-access support.
Pathophysiology
Homelessness and displacement expose individuals to chronic stress, trauma, victimization risk, and interrupted care, all of which worsen psychiatric symptoms and physical health outcomes. Co-occurring serious mental illness and substance-use disorders are common and can create cyclical instability.
Repeated housing loss erodes social support and treatment continuity, increasing emergency utilization and reducing long-term recovery probability without integrated interventions.
Classification
- Housing instability factors: Economic shocks, legal displacement, discrimination, and inadequate affordable housing.
- Displacement-legal-status domain: Refugee and asylum-seeker pathways differ in legal recognition and entitlement timing, influencing service access and continuity planning.
- Homelessness-contributor domain: Poverty, affordable-housing shortage, unaffordable health care, domestic violence, SUD burden, and persistent mental illness risk.
- Risk-matrix domains: Economic pressure, health burden, family conflict/violence exposure, social isolation, legal actions (eviction/foreclosure), disaster displacement, policy trends (gentrification), substance misuse, and limited support-service access.
- Clinical vulnerability factors: Serious mental illness, SUD, trauma exposure, and untreated comorbidity.
- Service access barriers: Transportation gaps, insurance limitations, fragmented systems, and rural scarcity.
- Clinical-access barrier cluster: Transportation limits, fragmented services, scheduling barriers, stigma, distrust, social isolation, and competing survival needs.
- Terminology-respect domain:
homeless,unsheltered,unhoused, andhouselessmay carry different lived meanings; assessment should include the person’s language preference. - Special-population domain: Veteran homelessness with PTSD/anxiety burden, family/child developmental risk during instability, and hidden rural homelessness with low service density.
- Low-threshold medical-home model: Walk-in/flexible access, street/shelter outreach, integrated primary-mental health care, on-site sustenance supports, and intensive cross-agency care management.
Nursing Assessment
NCLEX Focus
Assess immediate safety, housing status, and co-occurring SMI/SUD together to guide realistic care planning.
- Assess current housing status, shelter safety, and immediate survival risks.
- Assess psychiatric symptom burden, suicidality, and substance-use severity.
- Assess practical disease-management feasibility in current housing context (for example medication storage, hygiene access, diet constraints, and wound-care follow-through).
- Assess access barriers: transportation, insurance, identification documents, and service eligibility.
- Assess practical care-access barriers specific to homelessness (appointment-keeping feasibility, trust/distrust patterns, and immediate survival-resource needs).
- For newly displaced/refugee clients, assess camp/route exposure risks (overcrowding, sanitation/water limitations, interrupted vaccination history, and delayed chronic-disease treatment).
- Ask the person what housing terminology they prefer and avoid identity labels that may increase stigma or disengagement.
- Assess social supports, legal stressors, and prior engagement with community resources.
- Assess readiness for motivational therapies and recovery-housing options.
- Assess emergency-utilization pattern and repeated hospitalization risk associated with untreated basic-needs burden.
- Assess criminal-legal involvement, arrest/victimization history, and emergency-department dependence patterns linked to housing instability.
- Assess special-population needs (veteran status, family/child safety-development concerns, and rural service-access limitations).
- Assess trauma-persecution history carefully (including torture or sexual/gender-based violence risk) and watch for somatic presentations (for example headaches, abdominal pain, nonspecific pain) that may mask mental distress.
Nursing Interventions
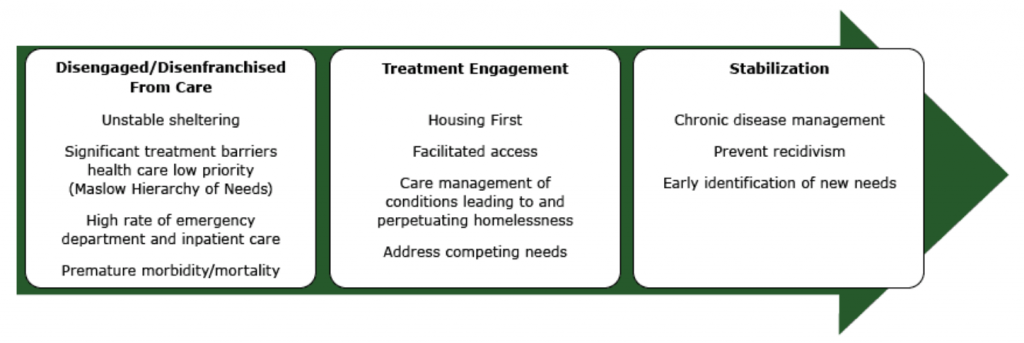 Illustration reference: OpenRN Nursing Mental Health and Community Concepts 2e Ch.17.2.
Illustration reference: OpenRN Nursing Mental Health and Community Concepts 2e Ch.17.2.
- Coordinate rapid linkage to housing, case management, and integrated behavioral health services.
- Use motivational interviewing and recovery-oriented planning for SUD/SMI stabilization.
- Advocate for trauma-informed, low-barrier care pathways across agencies.
- Collaborate with social work, legal aid, and public programs for benefits and transport access.
- In outreach/community settings, integrate immediate practical care (for example wound management, immunization linkage, and basic health checks) with mental-health triage to improve trust and follow-up.
- Use qualified interpreters with dialect/gender sensitivity when possible, and explain confidentiality limits clearly to reduce fear that testing results will affect immigration/asylum processes.
- Support continuity through follow-up touchpoints and community partner communication.
- Use low-threshold care design when possible (walk-in capacity, outreach encounters, and same-site integrated services).
- For children/families experiencing homelessness, coordinate school-health and case-management linkage early to support enrollment continuity, safety, and developmental follow-through.
- Coordinate access to immediate sustenance supports (food vouchers, hygiene kits, clothing, bus passes, and transport assistance) as part of clinical stabilization.
- Partner with refugee-resettlement and specialist support agencies to align infectious-disease screening, immunization catch-up, trauma services, and legal-social navigation.
- Transition clients to traditional primary-care settings when housing and self-care stability improve, while maintaining continuity safeguards.
- Use shelter/drop-in-center/mobile-clinic intake partnerships to reduce first-contact barriers and accelerate referral completion.
- Refer eligible clients to recovery housing programs that pair stable placement with counseling/support services.
- Coordinate with local/state/federal agencies for funding pathways that expand supportive housing, integrated SUD treatment, and rural outreach capacity.
Fragmentation Risk
Isolated referrals without coordinated follow-up often fail for clients facing multiple structural barriers.
Pharmacology
Medication effectiveness depends on stable access, storage feasibility, and follow-up continuity. Nursing care should prioritize practical adherence supports, regimen simplification where possible, and integrated monitoring with outreach-based services.
Clinical Judgment Application
Clinical Scenario
An unhoused client with bipolar disorder and alcohol use reports repeated shelter loss, missed medication doses, and recurrent emergency visits.
- Recognize Cues: Clinical instability is linked to housing and access disruption.
- Analyze Cues: SMI/SUD and structural barriers are reinforcing each other.
- Prioritize Hypotheses: Immediate priorities are safety, housing linkage, and treatment continuity.
- Generate Solutions: Build integrated plan with outreach psychiatry, case management, and recovery housing referral.
- Take Action: Activate interdisciplinary coordination and short-interval follow-up.
- Evaluate Outcomes: Reduced crisis visits and improved medication continuity.
Related Concepts
- substance-use-disorders - Frequent co-occurring condition in unstable housing contexts.
- dealing-with-addiction - Recovery supports are essential for housing stability.
- community-needs-in-mental-health-care - Social determinants framework for planning.
- collaboration-and-coordination-of-care - Cross-sector coordination drives outcomes.
- ptsd-and-veteran-trauma - Veteran trauma burden can increase homelessness risk and requires targeted referral pathways.