Measurement of Clinical Judgment
Key Points
- Clinical judgment is a progressive competency assessed pre-licensure and refined in practice.
- NCSBN uses the Clinical Judgment Measurement Model (CJMM) to evaluate safe entry-level decision-making.
- Next-generation NCLEX formats assess cue recognition, prioritization, action, and evaluation.
- CJMM measurement design emphasizes psychometric rigor for standardized, high-stakes exam decisions.
- PMH nursing requires applying measured judgment to complex psychosocial and medical data sets.
- NCSBN workforce/practice surveys (typically biennial) inform exam blueprints, curriculum priorities, and workforce planning.
- Layered CJMM reasoning requires reassessment loops when needs are unmet or partially met and integrates environment plus nurse factors.
- NCLEX-RN is a safety-oriented decision exam emphasizing acuity change management, prioritization, and resource use over rote recall.
Pathophysiology
This concept evaluates cognitive and reasoning performance rather than disease mechanisms. Clinical judgment quality influences patient safety, particularly in PMH contexts where psychosocial and physiologic cues may overlap.
Measurement frameworks aim to capture real-world reasoning under uncertainty and changing conditions.
Classification
- Model framework: CJMM steps from cue recognition through outcome evaluation.
- Layered architecture: Broad judgment context (layers 0-1), hypothesis cycle (layer 2), six cognitive skills (layer 3), and contextual modifiers (layer 4).
- Decision-model comparison: Decision trees and PICOT structure reasoning/inquiry, while CJMM is tailored for nursing clinical-judgment measurement in care decisions.
- Assessment formats: Multiple response, drag-and-drop, highlight, bow-tie, and trend items.
- Interactive-format domain: Case studies and stand-alone items may use bow-tie, drag-and-drop, drop-down, extended multiple response, matrix, highlight/specify, and split-screen visualization.
- Competency domains: Interpretation, prioritization, intervention selection, and reassessment.
- Regulatory-governance domain: Nurse Practice Acts define legal scope/licensure requirements by jurisdiction, and NCSBN coordinates cross-jurisdiction regulatory functions.
- Exam-development domain: Practice-analysis research and survey data are used to update NCLEX content emphasis and testing methods.
- NCLEX client-needs domain: Management of care, pharmacological/parenteral therapies, physiologic adaptation, reduction of risk potential, safety/infection control, health promotion/maintenance, psychosocial integrity, and basic care/comfort.
- Layer 4 modifier domain: Environmental factors (setting, resources, risk burden, time pressure, cultural context) and individual nurse factors (knowledge, skill, experience, candidate characteristics) shape outcomes.
- Expertise progression domain: Early practice relies on explicit layered reasoning; with expertise, prioritization becomes more rapid but still cyclical.
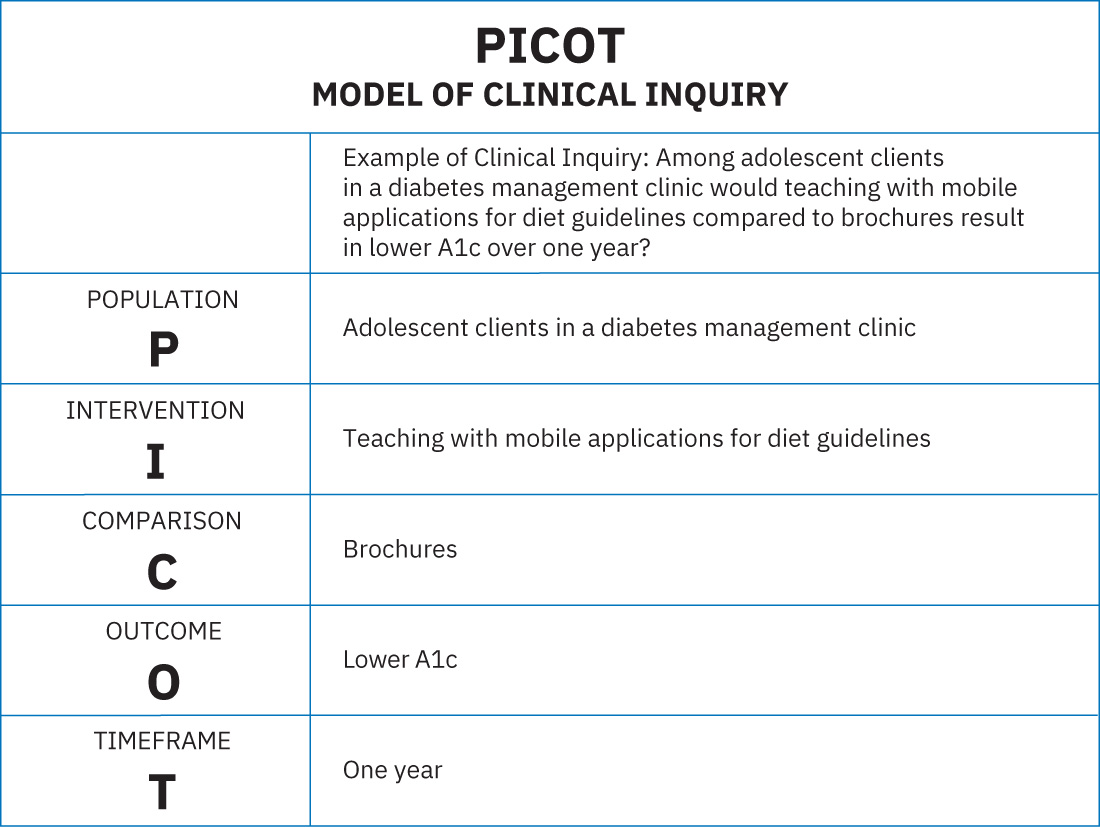 Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.28.2.
Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.28.2.
Nursing Assessment
NCLEX Focus
Read every item as a safety-prioritization task; identify unstable cues before selecting interventions.
- Assess whether presented data are primary or secondary and clinically relevant.
- Assess priority threats using physiologic safety and psychosocial risk framing.
- Assess expected versus unexpected findings in evolving scenarios.
- Assess how changing cues alter previously selected hypotheses.
- Assess whether selected actions remain appropriate after new data appear.
- Assess contextual modifiers (environment/resource/time-pressure and nurse-level factors) before final action selection.
- Assess question stems as dynamic safety problems requiring cue reprioritization when condition changes are introduced.
Nursing Interventions
- Use structured reasoning steps explicitly when solving scenario-based problems.
- Prioritize high-risk cues before lower-acuity psychosocial findings.
- Practice item deconstruction to distinguish distractors from safety-relevant data.
- Re-evaluate decisions when trend data indicate deterioration.
- Translate exam reasoning habits into bedside handoff and care-planning workflows.
- Practice with adaptive NGN-style scenarios and partial-credit item logic to improve test-day performance consistency.
- Use collaboration-oriented reasoning aligned with QSEN domains (person-centered care, teamwork, EBP, QI, safety, informatics) for PMH case responses.
Format Trap
Question format can distract from core safety reasoning; focus on client condition progression, not item style.
Pharmacology
Medication cues on judgment assessments often test adverse-effect recognition, interaction risk, and treatment prioritization. Nurses should integrate pharmacologic knowledge with trend interpretation and safety-first escalation decisions.
Clinical Judgment Application
Clinical Scenario
An NCLEX-style PMH item presents rising autonomic instability, altered behavior, and antipsychotic exposure with evolving labs.
- Recognize Cues: Identify unstable vital/lab trends and medication context.
- Analyze Cues: Distinguish likely emergent reaction from baseline psychiatric symptoms.
- Prioritize Hypotheses: Select life-threatening hypothesis first.
- Generate Solutions: Choose immediate stabilization and escalation actions.
- Take Action: Implement high-priority intervention sequence.
- Evaluate Outcomes: Reassess trends and revise plan based on response.
Related Concepts
- developing-critical-thinking-skills-in-nursing - Cognitive foundation for safe judgment.
- nursing-assessment-and-clinical-tools - Structured tools support better cue processing.
- nursing-process-in-psychiatric-mental-health-care - Operational model for judgment in PMH settings.
- integration-of-research-and-evidence-based-standards - Evidence informs safer decision models.