Diversity, Equity, and Inclusion
Key Points
- DEI strengthens nursing care quality by improving fairness, trust, and representation.
- Equality provides the same support; equity provides support based on need and barriers.
- Structural and interpersonal barriers drive disparities across race, identity, disability, and socioeconomic status.
- Communication quality determines whether DEI values translate into real clinical outcomes.
Pathophysiology
Health inequity is driven by social and structural conditions that increase chronic stress, reduce access, and delay treatment. In psychiatric care, inequity compounds symptom burden and worsens continuity outcomes.
Inclusive systems reduce harm by improving early access, culturally safe communication, and trust in care pathways.
Classification
- Justice domains: Equality (same allocation) versus equity (fair opportunity via tailored support).
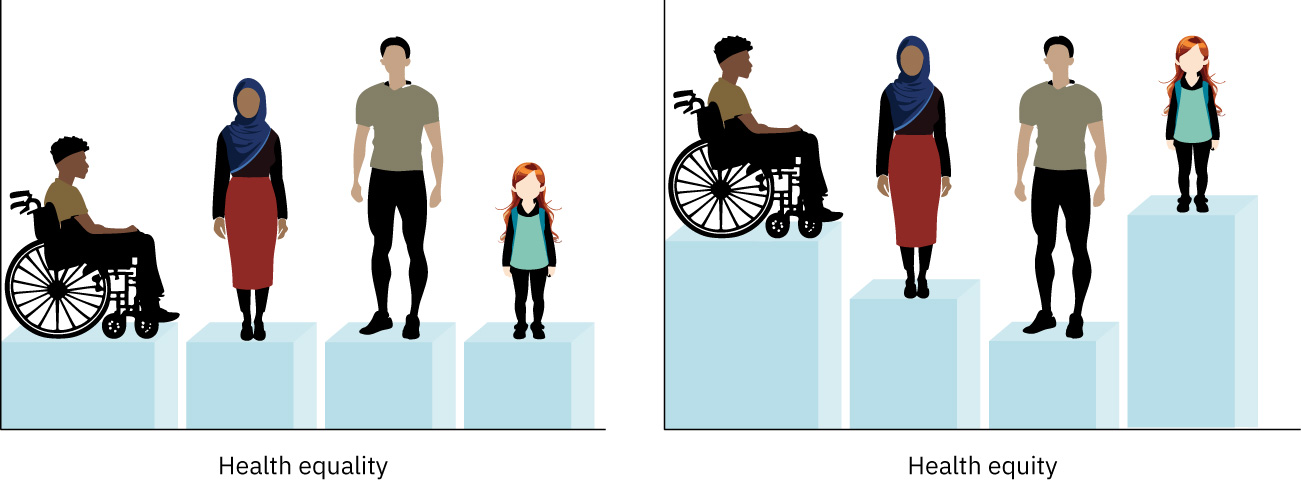 Illustration reference: OpenStax Clinical Nursing Skills Ch.5.
Illustration reference: OpenStax Clinical Nursing Skills Ch.5.
- Level-of-action domain: DEI is primarily organizational/structural, while cultural competence is enacted at the individual clinician level.
- Social justice domain: Equal rights, equal treatment, and equitable opportunities across societal structures, including respect for dignity, autonomy, security, and safety through fairness and unbiased evidence-based decisions.
- Race and racism domains: Race is socially constructed; racism imposes a hierarchy and produces unequal treatment and opportunity.
- Religion/spirituality domain: Spiritual beliefs may directly shape care acceptance (for example transfusion refusal, medication limits, diet, and end-of-life preferences).
- Barrier domains: Racism, bias, stereotyping, cultural imposition, cultural blindness, and culture conflict.
- Identity and access domains: Age, gender identity, sexual orientation, disability, education level, physical/sensory characteristics, socioeconomic status, and veteran status.
- Communication domains: Language access, health literacy, respectful identity-informed interaction.
- Privilege domain: Unearned social advantage tied to identity (for example race, gender, class, language, or ability) can shape access, trust, and treatment pathways.
- Agent-target framework domain: Dominant agent groups can benefit from systems that marginalize target groups through discrimination, exclusion, or exploitation.
- Systemic-oppression domain: Racism, sexism, ableism, ageism, language discrimination, and related structures can operate across policy, institution, and interpersonal levels.
- Decolonization domain: DEI practice includes challenging Eurocentric/colonial assumptions in care, education, and research while valuing diverse knowledge and healing traditions.
- Bias-reinforcement domain: In-group favoritism, out-group homogeneity assumptions, confirmation bias, media framing, limited cross-group contact, and cognitive-efficiency shortcuts can intensify stereotypes.
- Generalization-stereotype projection domain: Flexible cultural generalizations can guide inquiry, whereas fixed projection-based stereotypes drive unfair judgment and internalized prejudice.
Nursing Assessment
NCLEX Focus
Assess social and communication barriers as core clinical risks, not optional context.
- Assess social determinants and structural barriers affecting access and adherence.
- Assess identity-informed needs (race/ethnicity, gender identity, orientation, disability, veteran status, age).
- Assess communication barriers including language, literacy, and accessibility requirements.
- Assess hearing and vision accommodation needs (for example captioned media, assistive print formats, Braille, or screen-reader support) before education and consent discussions.
- Assess age-related undertreatment risk (for example pain, depression, or treatment denial assumptions).
- Assess gender and orientation safety climate, including pronoun preferences and prior discrimination history.
- Assess for gender-bias patterns in symptom attribution (for example emotional labeling of physical complaints) that can delay diagnosis and treatment.
- Assess religious/spiritual preferences that may affect medication, transfusion, diet, and end-of-life decisions.
- Assess spiritual decision factors with structured prompts (for example FICA: faith, importance, community, and address-in-care).
- Assess experiences of discrimination, prejudice, and mistrust impacting engagement.
- Assess race- and ethnicity-linked distrust risks tied to historical inequities and prior harmful encounters.
- Assess race- and ethnicity-linked disparity patterns (for example infant mortality or early cardiometabolic mortality trends) when planning outreach and prevention priorities.
- Assess organizational gaps (forms, equipment, policies) that hinder inclusion.
- Assess poverty, housing instability, transport barriers, and insurance constraints that block follow-through.
- Assess whether language services, forms, and educational materials are actually available for the local population profile.
- Assess education-level barriers that reduce preventive-care uptake and informed decision-making.
- Assess team-level barriers to diversity sensitivity, including low exposure to diverse groups, stereotype-based assumptions, and unexamined personal bias.
- Assess social-identity and privilege patterns that may influence nurse-client power dynamics and communication trust.
- Assess whether institutional norms/policies reinforce agent-group perspectives while suppressing target-group language, history, or care priorities.
- Assess whether bias-reinforcing factors (limited interaction, stereotype-confirming media exposure, and confirmation bias) are shaping team decisions.
Nursing Interventions
- Deliver inclusive, person-centered communication with identity-respect practices.
- Use interpreters and accessible materials to reduce communication inequity.
- Use trained medical interpreters (on-site or remote) for limited-English-proficiency encounters and avoid using family members as interpreters for clinical decision conversations.
- Use identity-affirming introductions (for example offering and asking pronouns) and document preferences consistently.
- Provide disability-access accommodations (for example ASL interpreters, accessible forms, or transfer equipment) rather than expecting patients to adapt.
- Integrate faith and spirituality preferences into care plans early (for example blood-product limits, diet, medication boundaries, and end-of-life choices).
- Challenge stereotyping and cultural imposition in care planning.
- Respond to culture conflict with humility-based negotiation that protects safety without dismissing core beliefs.
- Escalate system-level cultural blindness issues (for example missing translated consent forms for prevalent local communities).
- Address racist or discriminatory behavior in clinical settings through immediate safety-focused escalation and policy-aligned reporting.
- Use race- and ethnicity-stratified quality data to target disparity reduction plans rather than applying one-size-fits-all interventions.
- Address social determinants through advocacy and interprofessional coordination to reduce disparity-driving nonmedical barriers.
- Convert plans into context-feasible steps (for example hygiene- or storage-dependent regimens) when housing or resource constraints make standard instructions unrealistic.
- During interpreted encounters, address the patient directly, use short plain-language statements, avoid idioms/jargon, and verify understanding with teach-back.
- For hearing barriers, reduce background noise and use modality-matched supports (for example captioned media, TTY/text pathways, and qualified sign-language services).
- For vision barriers, optimize lighting and provide audio, large-print, magnification, screen-reader, or Braille options based on patient preference.
- Operationalize interpreter workflow: allow extra time, use one question at a time, document interpreter identity, and consider same-gender interpreter requests for sensitive discussions.
- Advocate for equity-focused policy and workflow improvements.
- Support ongoing cultural-competence education rather than one-time training.
- Track disparity patterns and partner with teams to close identified gaps.
- Use decolonizing DEI strategies by co-designing care approaches with affected communities and integrating diverse knowledge systems where clinically safe.
- Use structured privilege reflection tools and guided dialogue to convert awareness into equity-focused behavior and policy action.
- Interrupt in-group favoritism and out-group assumptions during planning/handoff by requiring evidence-based, person-specific reasoning.
- Use language access and health-literacy supports as core equity interventions to reduce privilege-linked communication advantage gaps.
Equality-Only Pitfall
Providing identical resources to unequal starting conditions can perpetuate inequity.
Pharmacology
Equitable pharmacologic care requires attention to access barriers, literacy, language, affordability, and follow-up capability. Nurses should tailor education and monitoring plans to each client’s context.
Clinical Judgment Application
Clinical Scenario
A clinic reports high psychiatric no-show rates in clients with limited English proficiency and low-income transportation barriers.
- Recognize Cues: Disparity pattern suggests structural barriers, not low motivation.
- Analyze Cues: Communication and access inequities are interrupting care continuity.
- Prioritize Hypotheses: Priority is equity-focused redesign of scheduling and communication workflows.
- Generate Solutions: Add interpreter-first outreach, transport supports, and flexible visit options.
- Take Action: Implement targeted interventions and staff training on inclusive communication.
- Evaluate Outcomes: Monitor follow-up rates, symptom outcomes, and disparity-gap reduction.
Related Concepts
- understanding-cultural-differences - Establishes culture and disparity fundamentals.
- ethical-practice-in-culture-and-diversity - Anchors DEI efforts in ethical nursing obligations.
- cultural-practice-in-nursing - Translates DEI principles into daily bedside practice.
- communication-within-the-health-care-team - Supports inclusive team coordination and handoff.
- collaboration-and-coordination-of-care - Connects equity goals with system-level care delivery.