Developmental Theories in Nursing Erikson Piaget Kohlberg and Freud Applied Comparison
Key Points
- Developmental theories provide structured lenses for age-appropriate nursing assessment and intervention.
- Erikson focuses psychosocial conflict resolution; Piaget focuses cognitive-processing progression.
- Kohlberg describes moral reasoning evolution; Freud describes psychosexual-stage assumptions and conflicts.
- Freud’s model frames early childhood personality organization through id, ego, and superego development and stage-sequenced drive control.
- Piaget’s stages guide progression from sensory-motor learning to abstract reasoning and should be paired with development-level communication.
- Kohlberg’s model organizes moral reasoning into preconventional, conventional, and postconventional levels; only a minority reach stable postconventional reasoning.
- Havighurst’s model adds a developmental-task lens: age-specific tasks should be achieved to support smoother progression to later stages.
- Clinical usefulness comes from practical application, not rigid stage labeling.
Pathophysiology
Developmental theories do not describe disease pathways directly; they organize expected changes in cognition, identity, relationships, and decision behavior. In practice, theory-informed assessment improves communication matching and reduces care-plan mismatch.
Classification
- Psychosocial lens (Erikson): Stage conflicts and adaptive identity/role outcomes across trust vs mistrust (0-1.5 years), autonomy vs shame/doubt (1.5-3 years), initiative vs guilt (3-5 years), industry vs inferiority (5-12 years), identity vs role confusion (12-18 years), intimacy vs isolation (18-40 years), generativity vs stagnation (40-65 years), and ego integrity vs despair (65 years and older).
- Cognitive lens (Piaget): Sensorimotor (birth to about 2 years), pre-operational (2-6 years), concrete operational (7-11 years), and formal operational (about 12 years and older) reasoning progression.
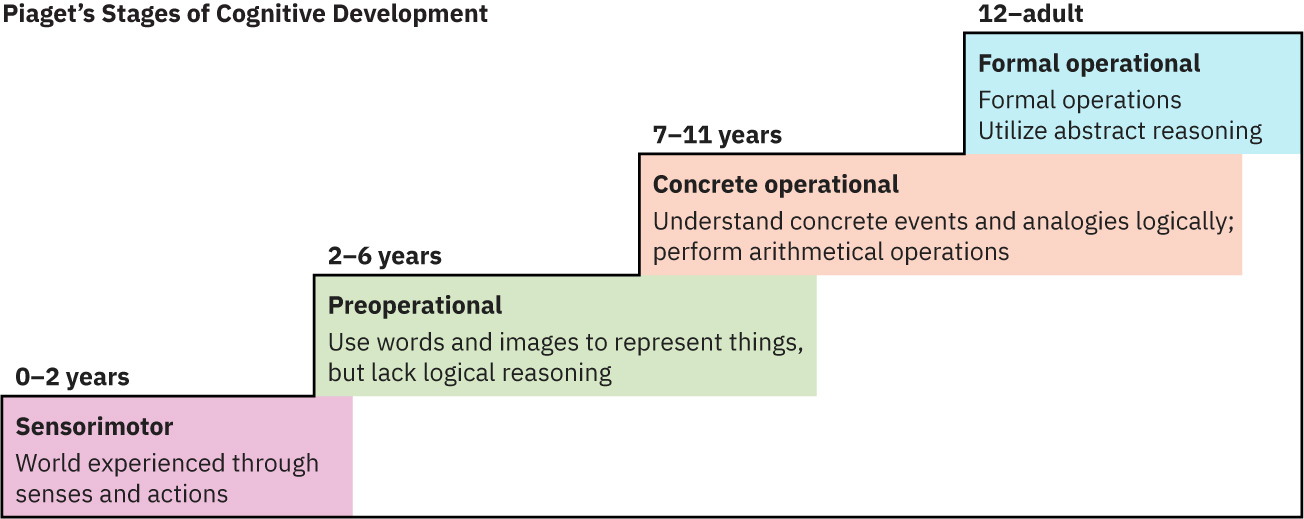 Illustration reference: OpenStax Fundamentals of Nursing Ch.38.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.38.2.
- Moral lens (Kohlberg): Preconventional (about ages 0-9; obedience/punishment then individual interest), conventional (about ages 10-15; interpersonal approval then authority/social-order duty), and postconventional (about age 16+; social contract then universal ethics), with only a minority reaching stable postconventional reasoning.
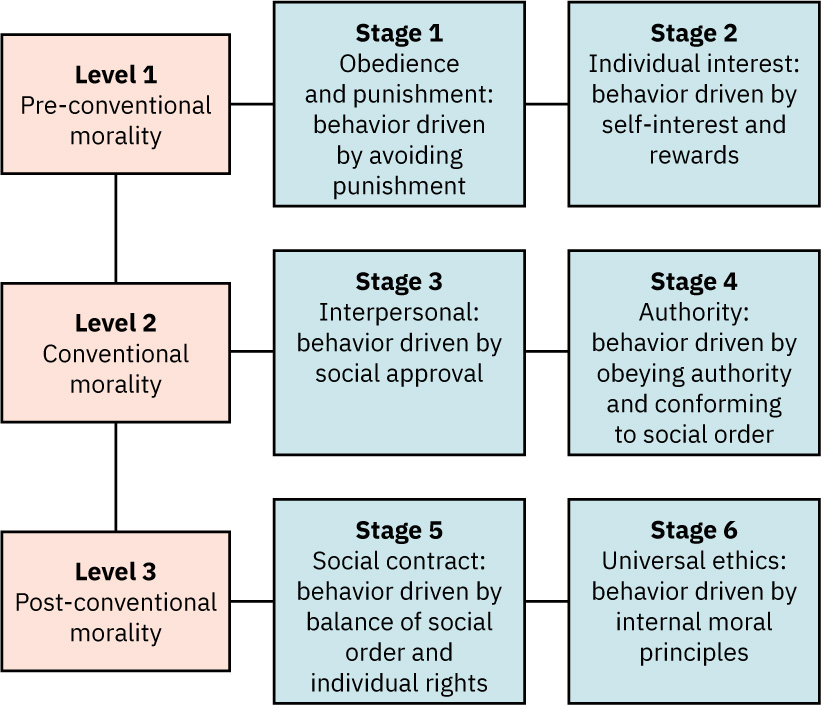 Illustration reference: OpenStax Fundamentals of Nursing Ch.38.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.38.2.
- Psychosexual lens (Freud): Stage-centered drive/conflict framework (oral 0-1, anal 1-3, phallic 3-6, latency 6-puberty, genital puberty-adulthood) linked to id-ego-superego dynamics and consciousness levels (unconscious, preconscious, conscious), with contested modern applicability.
- Task-completion lens (Havighurst): Stage-linked developmental tasks (for example early childhood language/toileting/foundation learning, later-childhood game/social independence tasks, adolescent puberty acceptance/intimacy preparation/career planning/value formation) where incomplete tasks raise risk for later adjustment difficulty.
Nursing Assessment
NCLEX Focus
Match education, consent discussion, and behavior expectations to developmental processing level.
- Assess psychosocial stage cues affecting adherence and coping.
- Assess whether unresolved earlier psychosocial conflicts (for example mistrust from inconsistent caregiving) are amplifying present care resistance or relational withdrawal.
- Assess cognitive level to tailor explanation complexity and concrete versus abstract teaching style.
- In preoperational children, assess symbolic role enactment (dramatic play) as a normal representational-thinking milestone.
- In pre-operational children, assess for magical thinking, animism, egocentrism, and centration that can produce prelogical self-blame (for example believing illness is their fault).
- Assess moral-reasoning style when conflict and value decisions emerge.
- Assess whether current decisions are primarily punishment-avoidant, approval-seeking, duty/order-focused, or principle-based to match counseling depth.
- In preconventional reasoning, assess for fear-driven symptom minimization/denial and for treatment acceptance based only on immediate personal benefit.
- In conventional reasoning, assess whether social-judgment concerns reduce disclosure of sensitive information.
- In adolescents, assess mismatch between emerging abstract reasoning and still-maturing impulse control when discussing risk decisions.
- Assess whether formal operational thinking is generalized or domain-specific, because abstract/hypothetical reasoning may be strong in one context and limited in another.
- Assess Freud-informed early-childhood behavior in context of emerging id/ego/superego control while avoiding rigid stage labeling.
- Assess whether theory-based expectations fit the individual’s cultural context, especially for identity and autonomy tasks in adolescence.
- Assess developmental mismatch between age and functional behavior that may need further evaluation.
- Assess whether age-expected developmental tasks are being achieved, because unresolved task completion can signal elevated risk for later adaptation problems.
- Use Piaget stage anchors when planning communication and instruction:
- Sensorimotor (birth to about 2 years)
- Preoperational (toddler through early school age)
- Concrete operations (about 7-11 years)
- Formal operations (about 12 years and older)
- In concrete-operational children, assess ability to follow multistep concrete instructions and solve practical problems while screening for difficulty with hypothetical reasoning.
Nursing Interventions
- Use stage-appropriate language and concrete-to-abstract teaching progression.
- For sensorimotor-stage children, support sensory exploration with safe toys and frequent language exposure (talking, reading, singing).
- For pre-operational children, prioritize play-based teaching, simple procedure explanations, and reassurance that illness events are not their fault.
- For pre-operational children, use symbolic play and concrete language to address fantasy-based fears while avoiding overreliance on abstract logic alone.
- For concrete-operational children, provide factual cause-effect teaching about health conditions and treatments.
- For concrete-operational children, use tangible examples (timelines, pill boxes, visual routines) rather than abstract “what-if” teaching alone.
- For formal-operational adolescents, use abstract discussion as appropriate and encourage participation in health-care decision-making.
- Do not assume universal formal-operational reasoning in all patients; verify comprehension in the decision context before escalating teaching complexity.
- For adolescents, frame risk counseling around real social scenarios (peer pressure, relationships, and immediate reward tradeoffs), not abstract warnings alone.
- Use Kohlberg-guided communication: explain why treatments/rules exist, reduce judgment during sensitive disclosure, and support informed autonomy for older adolescents/families.
- For higher-level moral conflict, discuss rights-versus-rules tradeoffs explicitly and support structured ethical reasoning rather than authority-only directives.
- Support autonomy and identity formation without unsafe overexposure.
- Incorporate family/caregiver coaching aligned with developmental tasks.
- Reframe challenging behavior through developmental context before punitive interpretation.
- Use Erikson-informed coaching for caregivers: balance independence support with developmentally appropriate guidance so autonomy and initiative are strengthened without shame or guilt reinforcement.
- Use Havighurst-informed planning to break stage goals into achievable tasks and reinforce mastery before advancing expectations.
Stage Determinism
Treating stages as fixed labels can overlook culture, trauma, neurodiversity, and individual variation.
Pharmacology
Medication adherence and side-effect interpretation are influenced by developmental cognition and psychosocial context; teaching should be adapted accordingly.
Clinical Judgment Application
Clinical Scenario
A 14-year-old with chronic illness rejects treatment, citing peer-image concerns and inconsistent reasoning about long-term risk.
- Recognize Cues: Identity conflict and evolving abstract reasoning.
- Analyze Cues: Developmental factors are driving nonadherence more than knowledge deficit alone.
- Prioritize Hypotheses: Preserve safety while strengthening autonomy-supportive engagement.
- Generate Solutions: Use adolescent-focused shared decisions and peer-sensitive education strategies.
- Take Action: Implement staged counseling and family-aligned support plan.
- Evaluate Outcomes: Improved adherence and more stable decision quality.
Related Concepts
- growth-vs-development-lifespan-milestones-and-play-patterns - Observable milestones that anchor theory use.
- atraumatic-care-and-developmentally-appropriate-communication - Communication approach adapted by stage.
- well-care-anticipatory-guidance-and-immunization-across-the-lifespan - Preventive visit structure supporting developmental guidance.
- developmental-theories-and-therapies - Psychiatric-depth theory integration.
- eriksons-stages-of-development - Detailed psychosocial stage content.
Self-Check
- Which clinical questions are best answered by Erikson versus Piaget frameworks?
- How does Kohlberg help interpret treatment-decision conflict?
- Why should theory-informed care avoid rigid stage assumptions?