Cognitive Behavioral Therapy
Key Points
- Cognitive behavioral therapy (CBT) is a structured, evidence-based psychotherapy that links thoughts, behaviors, and emotions — changing how a person thinks changes how they feel and act
- Core principle: Emotional distress stems from distorted thinking patterns (cognitive distortions) that can be identified, challenged, and reframed
- Indications: Depression, anxiety disorders, OCD, PTSD, eating disorders, alcohol/drug use disorders, chronic pain, severe mental illness
- Neurodevelopmental context: Adapted CBT may help autistic clients manage coexisting anxiety/depression using concrete, structured coping practice.
- In pediatric care, psychotherapy is selected by developmental level and often paired with medication when disorder severity requires combined treatment.
- Research shows CBT is as effective as or more effective than psychiatric medications for many conditions
- In depressive disorders, psychotherapy can be used alone for mild episodes or combined with medication for moderate-to-severe episodes; meaningful gains are often seen over about 10-15 sessions
- The nurse’s role is supportive — reinforcing CBT homework, modeling therapeutic behaviors, and teaching coping skills
Core Principles
CBT is grounded in three interrelated principles:
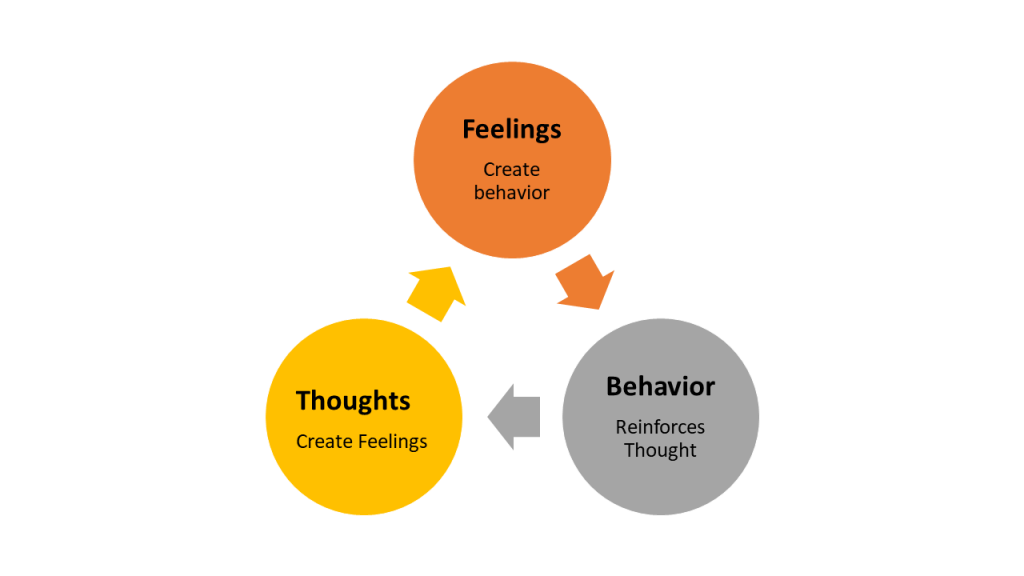 Illustration reference: OpenRN Nursing Mental Health and Community Concepts 2e Ch.10.3.
Illustration reference: OpenRN Nursing Mental Health and Community Concepts 2e Ch.10.3.
| Principle | Strategy | Rationale |
|---|---|---|
| Thoughts | Recognize cognitive distortions; reframe to match reality | What we think affects how we feel and act |
| Behavior | Understand motivations; modify negative behavioral patterns | How we behave affects how we think and feel |
| Emotion | Learn coping techniques; apply problem-solving skills | What we feel affects how we think and act |
CBT process: Clients identify negative automatic thoughts → examine evidence for and against → develop more balanced alternative thoughts → practice behavioral skills between sessions (“homework”)
CBT Modalities
Cognitive Behavioral Therapy (CBT)
- Goal: Identify and restructure distorted thinking patterns (cognitive distortions)
- Techniques: Role-play, journaling, exposure exercises, behavioral experiments
- Behavioral activation: Build a graded activity plan (specific measurable activities, easiest first, then step-up difficulty) to reverse withdrawal and isolation patterns
- Indications: Depression, anxiety, panic disorder, phobias, bulimia nervosa, PTSD
- Time-limited: Typically 12–20 sessions; skill-based, with homework between sessions
- CBT clinicians focus on current situations and thought patterns rather than past events
Dialectical Behavior Therapy (DBT)
- Goal: Develop distress tolerance, emotional regulation, and interpersonal effectiveness
- Core skills: Mindfulness, distress tolerance, emotional regulation, interpersonal effectiveness
- Structure: Skills groups plus individual therapy sessions, commonly with mindfulness practice
- Indications: Borderline personality disorder, substance misuse, eating disorders, suicidal behavior
Acceptance and Commitment Therapy (ACT)
- Uses positive reinforcement and counterconditioning (graduated exposure + relaxation)
- Helps clients accept negative emotions rather than fight them while committing to value-aligned behavior
- Indications: Anxiety, OCD, depression, stress, psychosis, substance use disorders
Mindfulness-Based Cognitive Therapy (MBCT)
- Combines cognitive therapy with meditation and mindfulness practices
- Effective for: Recurrent depression, anxiety, bipolar disorder
- Teaches clients to observe thoughts without reacting automatically
Milieu Therapy
- A therapeutic community environment that provides safety, structure, and consistent routine
- Allows clients to learn and practice behaviors in real-time social interactions
- Key components: Staff modeling of desired behaviors, community accountability, supported decision-making, therapeutic communication
Exposure Therapy
A CBT subtype specifically for anxiety and phobia:
- Exposure therapy: Directly confronts feared situations or objects to reduce avoidance
- Systematic desensitization: Graduated exposure at a slow pace combined with relaxation techniques
- Used for: Social anxiety disorder, specific phobias, PTSD, OCD
For OCD, a core CBT variant is exposure and response prevention (EX/RP or ERP): clients are exposed to obsession-triggering cues and then coached to refrain from the usual compulsion, allowing anxiety to decrease without ritual completion. EX/RP is used as a primary psychotherapy or as an add-on when medication response is incomplete.
Nursing Role in Behavioral Therapy
The nurse is not the primary CBT therapist but plays a critical supportive role:
- Observe and document: Behavioral patterns, mood shifts, and responses to interventions
- Reinforce CBT skills: Encourage journaling, thought records, and homework completion
- Model therapeutic behaviors: Demonstrate calm, non-judgmental communication
- Monitor suicidality: Antidepressants and CBT together may initially increase awareness of suicidal ideation — monitor closely when therapy starts or changes
- Collaborate: Coordinate with psychiatrists, psychologists, and social workers as interprofessional team member
- Group therapy facilitation: Support clients participating in group CBT sessions
Nurse Scope
Nurses do not conduct formal CBT but implement milieu therapy, teach coping skills, and reinforce what therapists prescribe. Advanced practice nurses (APRNs) may provide individual or group CBT if licensed.
Related Concepts
- therapeutic-communication — Foundation of the therapeutic nurse-client relationship in behavioral therapy
- anxiety-related-disorders — Primary CBT indication; exposure therapy for phobias and GAD
- trauma-informed-care — CBT/DBT approaches adapted for trauma survivors
- substance-use-disorders — CBT and DBT used for addiction relapse prevention
- psychotropic-medications — CBT often combined with antidepressants or anxiolytics for optimal outcomes
- mental-health-and-mental-illness — Biopsychosocial framework for mental illness treatment
Self-Check
- A nurse is working with a patient who states, “I always fail at everything — there’s no point in trying.” Using CBT principles, what cognitive distortion does this statement represent, and what technique would a therapist use to address it?
- A patient with borderline personality disorder is enrolled in a DBT program. What four skill modules would DBT teaching address?
- What is the nurse’s primary role when caring for patients who are receiving CBT from a licensed psychologist?