Person Centered Care Foundations Shared Decision Making and Self Management
Key Points
- Person-centered care integrates patient goals, values, social context, and beliefs into care planning.
- Shared decision-making and self-management support improve outcomes in chronic and complex care.
- Physical, emotional, and spiritual needs should be assessed together rather than in isolation.
- Developmental stage and life events can change care preferences and barriers over time.
- A caring relationship (rapport and trust) with compassionate presence is foundational for effective whole-person assessment and planning.
- Planning should explicitly include identity-affirming preferences and privacy/dignity expectations, especially when prior healthcare experiences reduced trust.
- Patient-centered plans can improve adherence, safety, and satisfaction while reducing avoidable tests, procedures, and readmissions over time.
- Effective patient-centered care values emotional well-being and physical comfort equally while integrating social, spiritual, and financial context.
- Family participation preferences and timely information sharing support informed decisions and better continuity.
Pathophysiology
Person-centered care is a care-delivery framework, not a disease mechanism. It shapes how nurses gather cues, prioritize problems, and co-create plans with patients and families. Better alignment between the care plan and patient priorities improves adherence, engagement, and continuity.
When care excludes preferences or context, distress rises and participation often falls. By contrast, person-centered planning supports trust, realistic goals, and safer decisions during changing clinical conditions.
Classification
- Historical foundation: Rogers-derived person-centered therapy principles influenced shared decision-making and modern person-centered nursing care.
- Patient-centered care: Emphasizes active patient participation, communication, and coordinated services.
- Person-centered care: Expands focus to social, cultural, and spiritual values with individualized goals and preferences.
- Holistic care: Integrates mind, body, and spirit, including complementary approaches when safe and appropriate.
- Operational tenets domain: Contemporary person-centered frameworks include shared decision-making and structured self-management support as core practice elements.
- SHARE process domain: AHRQ SHARE is a five-step shared decision-making approach that keeps patient participation central throughout decision formation and follow-up.
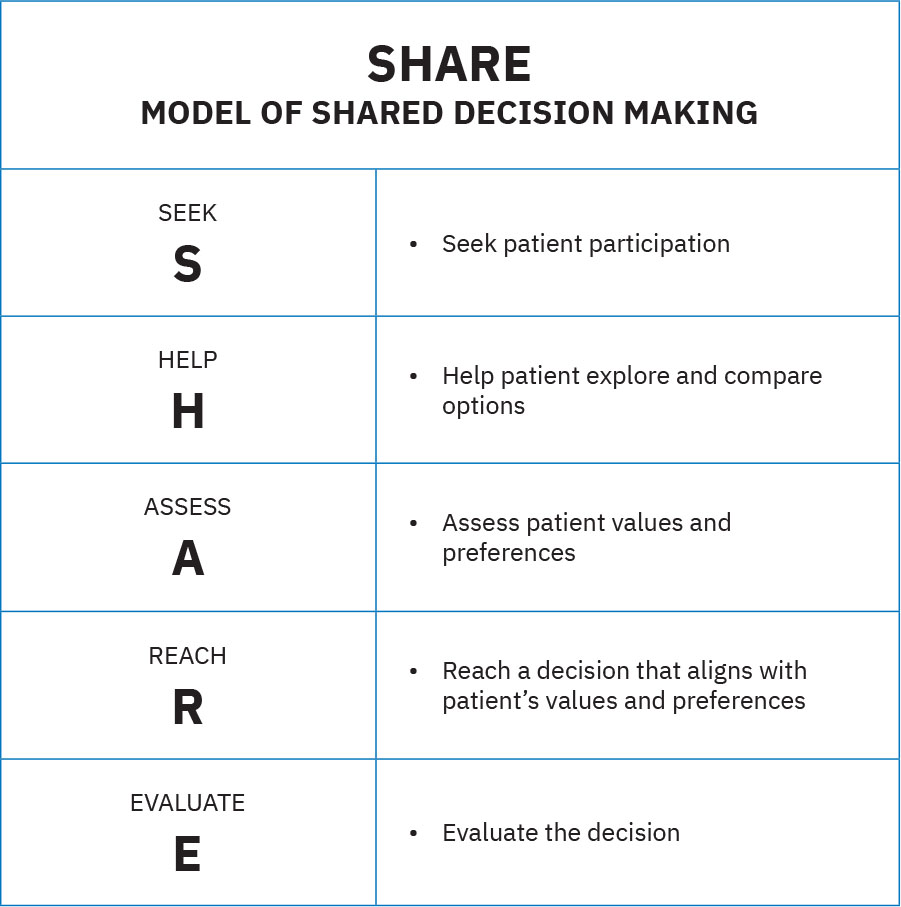 Illustration reference: OpenStax Fundamentals of Nursing Ch.15.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.15.2. - Patient-centered attribute domain: Include family as preferred care partners, share information promptly, respect culture and socioeconomic context, and deliver the right care at the right time in the right place.
Nursing Assessment
NCLEX Focus
Priority questions test whether the nurse elicits values and preferences before finalizing interventions.
- Assess patient goals, beliefs, and preferred role in shared decision-making.
- Assess prior healthcare harms or mistrust that may reduce engagement unless trust is actively rebuilt.
- Assess patient preference for transparent information sharing (risks/benefits/alternatives) and written action plans.
- Assess access and readiness for digital engagement tools (for example patient portals) to support ongoing result review and treatment participation.
- Assess physical and physiologic priorities such as pain, mobility, elimination, and safety.
- Assess emotional factors such as fear, grief, anxiety, and readiness for self-management.
- Assess procedure-specific fear barriers (for example claustrophobia before MRI) early so alternatives or supports can be arranged.
- Assess spiritual preferences, practices, and desired supports.
- Assess priority order using physiologic-first safety logic (Maslow-based sequencing) before higher-level social/esteem goals.
- Assess identity-affirming care preferences (for example name/pronoun use and privacy boundaries) and incorporate them into planning.
- Assess developmental and life-event factors that may alter coping, consent, and treatment participation.
- Assess safety/security context including insurance coverage, financial strain, and available social supports that may affect plan feasibility.
- Assess who the patient defines as family/support system (including chosen family) and who is permitted to receive private health information.
- Assess prior beliefs and previous negative healthcare experiences or trauma that may alter acceptance of recommended plans.
- Assess practical constraints (for example caregiver roles, work obligations, transportation, or home-support limits) that may alter feasible care options.
- Assess whether the patient wants family/support persons present during rounds, shift-report participation, and treatment discussions.
- Assess what matters most to the patient and whether current orders and care goals remain aligned with documented directives.
Nursing Interventions
- Use shared decision-making to compare options and align plans with patient priorities.
- Use plain, jargon-free language and transparent risk/benefit discussion so patients can make autonomous decisions.
- Teach self-management skills with clear language and return-demonstration where needed.
- Co-create written, personalized action plans that connect treatment steps to patient-defined life goals.
- Use structured follow-up interactions after procedures, test results, or medication changes to reduce adverse events and strengthen continuity.
- Use integrated-service pathways when available so treatment options, well-being goals, and comprehensive needs are planned together.
- Coordinate interdisciplinary resources for complex physical, emotional, and spiritual needs.
- Involve family or legal decision makers (including designated medical power of attorney when applicable) according to patient preference and capacity.
- Link patients/families to financial and social-support resources early when safety/security needs threaten adherence.
- Maintain a welcoming identity-affirming environment and treat privacy/dignity protections as non-negotiable plan elements.
- Respect confidentiality boundaries by sharing information only with patient-approved individuals.
- Use qualified medical interpreters when language discordance could limit accurate preference elicitation or informed choice.
- Reassess goals after major transitions, new diagnoses, or significant life events.
- Coordinate trauma-informed or grief-support referrals when previous loss or trauma interferes with healing and participation.
- Use caring behaviors such as active listening, eye contact, therapeutic touch when appropriate, and culturally respectful emotional support to strengthen trust.
- Invite patient-designated family/support persons into rounds or handoff discussions when the patient prefers this participation.
- Provide timely updates to the patient and designated support persons so decisions remain informed and value-concordant.
Preference-Plan Mismatch
Plans that ignore values, developmental context, or spiritual preferences increase nonadherence and avoidable poor outcomes.
Pharmacology
Pharmacologic treatment remains important, but outcomes improve when medication plans are built into a person-centered strategy that supports understanding, adherence, and ongoing self-management.
Clinical Judgment Application
Clinical Scenario
A postoperative patient reports uncontrolled pain, fear of another procedure, and requests prayer support before treatment decisions.
- Recognize Cues: Physical, emotional, and spiritual needs are all active.
- Analyze Cues: Single-domain planning will likely fail.
- Prioritize Hypotheses: Immediate priorities are pain control, safety, and trust-building.
- Generate Solutions: Use shared decision-making, add spiritual support, and provide clear self-management teaching.
- Take Action: Implement the interdisciplinary plan and document preferences.
- Evaluate Outcomes: Participation and symptom control improve.
Related Concepts
- person-and-family-centered-care - Expands inclusive family and identity-sensitive care implementation.
- organizational-culture-patient-centered-collaborative-and-safety-frameworks - Connects person-centered goals to team and system workflows.
- self-management-and-collaborative-chronic-care - Operationalizes long-term self-management support.
- holistic-health-and-interventions - Adds whole-person and complementary intervention strategies.
- spiritual-assessment-and-patient-centered-care-planning - Provides structured spiritual inquiry and planning.
Self-Check
- How is person-centered care broader than patient-centered care in daily nursing decisions?
- Which findings signal the need to update a care plan after a life event?
- Why should self-management support be treated as an ongoing process rather than a single education event?