Motivational Coaching and SMART Goals in Nursing Education
Key Points
- Motivation influences whether education becomes sustained behavior change.
- Intrinsic motivation comes from internal values; extrinsic motivation uses external rewards.
- Coaching supports collaborative problem-solving rather than directive instruction alone.
- SMART goals improve clarity, feasibility, and accountability in self-care plans.
- Discharge planning is stronger when SMART goals are co-built with patient values, caregiver capacity, and real resource limits.
- Nurse-coaching partnerships use identify-assess-plan-evaluate cycles to convert wellness goals into sustained behavior change.
- Nonjudgmental, non-shaming coaching improves behavior-change engagement and persistence versus blame-based counseling.
- Stage progression is often nonlinear; relapse movement is expected and should trigger plan adjustment, not failure labeling.
- A 0-to-10 confidence rating helps quantify self-efficacy and guides how aggressively to advance or revise the plan.
Pathophysiology
Low motivation reduces adherence even when understanding is adequate. Structured coaching and goal-setting convert abstract advice into actionable routines, reducing relapse risk and improving health behavior consistency.
Classification
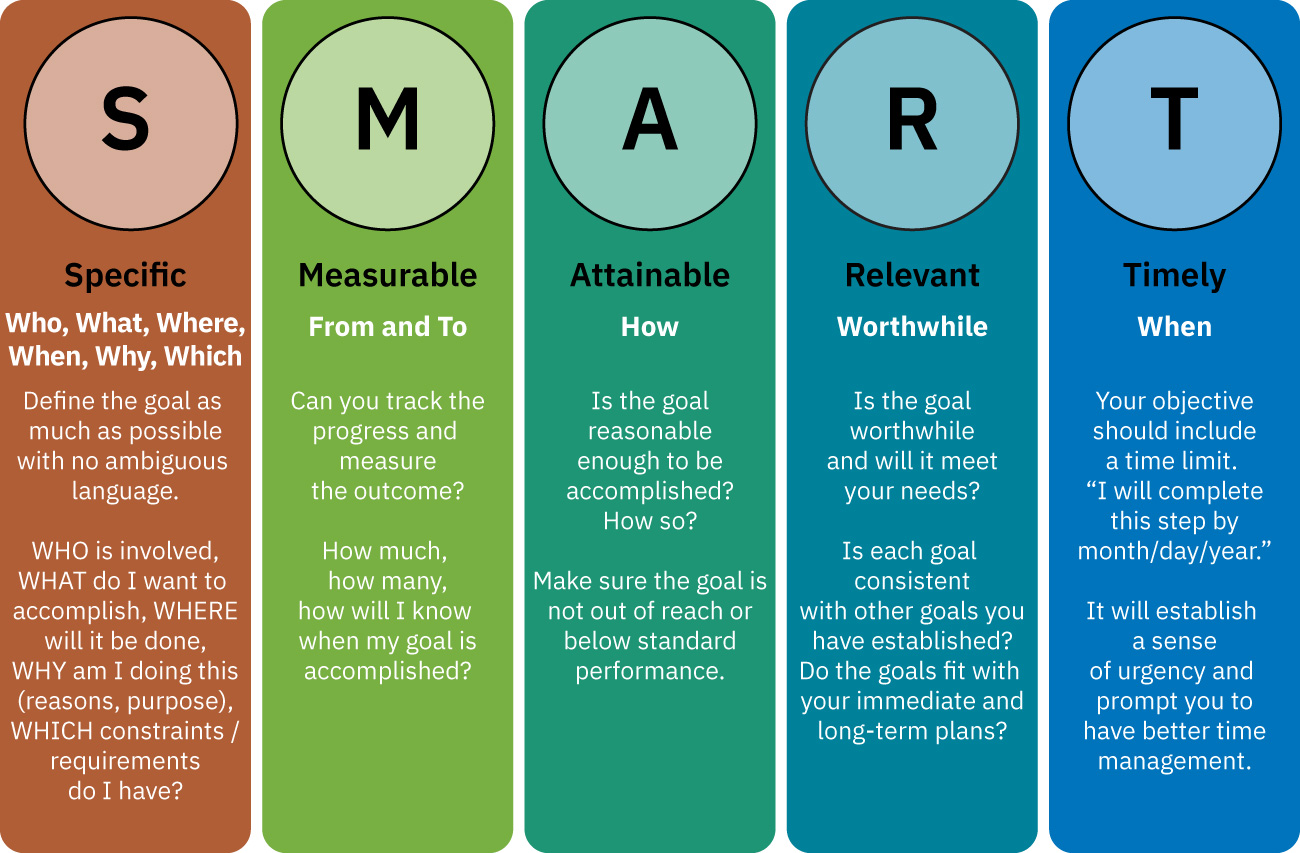 Illustration reference: OpenStax Clinical Nursing Skills Ch.1.
Illustration reference: OpenStax Clinical Nursing Skills Ch.1.
- Intrinsic motivation: Behavior driven by internal meaning, health values, or self-fulfillment.
- Extrinsic motivation: Behavior driven by external incentives or outcomes.
- TTM stage alignment: Precontemplation, contemplation, preparation, action, and maintenance require different coaching intensity.
- TTM flow characteristics: Stage progression is often nonlinear with forward/backward movement; stages are not skipped even when relapse occurs.
- TTM timing windows: Precontemplation (no intent within 6 months), contemplation (intent within 6 months), preparation (intent within 30 days with first steps), action (<6 months behavior change), maintenance (>6 months), and termination (no relapse temptation with full confidence).
- HBM-guided counseling overlay: Perceived susceptibility/severity, perceived benefits/barriers, cues to action, and self-efficacy shape readiness and adherence.
- Coaching process: Guided collaboration to identify barriers, strengths, and realistic next steps.
- SMART structure: Specific, measurable, attainable, relevant, and timely goals.
- Nurse-coaching wellness cycle: Patient-centered coaching that creates safe space for goal exploration and uses iterative identifying, assessing, planning, and evaluating steps.
Nursing Assessment
NCLEX Focus
Determine what matters to the patient before proposing behavior-change steps.
- Assess motivational drivers and current stage of willingness.
- Assess stage-specific change language and timeline cues (for example no intent in six months, considering change, or commitment within 30 days).
- Assess perceived threat and barrier-benefit balance before setting goals (HBM lens).
- Assess prior behavior-change attempts and barriers to success.
- Assess confidence, social supports, and practical constraints.
- Assess readiness numerically using 0-to-10 importance and confidence ratings to establish a baseline for reevaluation.
- Assess work-life-load barriers (for example caregiving burden, overtime demands, and role overload) that limit behavior-change follow-through.
- Assess whether family/caregiver support and community resources can realistically sustain the proposed goal after discharge.
- Assess relapse triggers and contingency resources before action plans are finalized.
- Assess whether goals are patient-owned versus externally imposed.
- Assess follow-up capacity for progress checks and reinforcement.
- Assess communication barriers and emotional-cognitive readiness before setting interaction goals.
- Assess readiness to engage in iterative coaching cycles and sustained reflection between visits.
Nursing Interventions
- Use open-ended questions to clarify patient priorities and concerns.
- During plan reevaluation, use open-ended prompts about goal execution, symptom trend since initiation, and unresolved barriers to sustain self-efficacy.
- Use nonjudgmental language and avoid shame-based framing when discussing lifestyle risks or prior unsuccessful attempts.
- Match intervention to stage of change (awareness-building in precontemplation; concrete action planning in preparation/action).
- Use stage-specific nursing goals: raise consciousness in precontemplation, resolve ambivalence in contemplation, build logistics in preparation, reinforce wins in action, and sustain trigger-management in maintenance.
- Use recurring low-burden follow-up prompts (brief calls/text reminders) when adherence depends on repeated cue-to-action reinforcement.
- Co-develop one high-impact SMART goal tied to patient values.
- Use nurse-coaching partnership behaviors (active listening, nonjudgmental reflection, and co-prioritization) to support long-term wellness and life-balance goals.
- Translate broad discharge intentions into SMART goals with concrete numeric targets and timeline checkpoints.
- Use SMART goals for therapeutic conversations when trust-building or education outcomes need explicit measurement.
- Convert vague goals into measurable language (for example, define exact frequency and timeframe instead of “once in a while”).
- Build concrete action steps, schedule, and monitoring method.
- Include boundary-setting and schedule-prioritization planning when work-home imbalance is the dominant barrier.
- Start with low-intensity, achievable behavior targets for sedentary or overwhelmed patients, then scale intensity as confidence and consistency improve.
- Reinforce progress with nonjudgmental feedback and problem-solving.
- If confidence remains below target, use follow-up probing (for example, “Why this number and not lower?”) to identify strengths and removable barriers before raising goal intensity.
- Normalize relapse risk and use setbacks as data for plan revision rather than treatment failure.
- Document and rehearse relapse-response steps (support contacts, trigger-avoidance strategies, and restart actions) so setbacks re-enter the change cycle quickly.
- Revise goals when barriers emerge rather than labeling failure.
Vague Goal Pitfall
Goals without measurable targets and timelines often fail despite patient intent.
Pharmacology
Medication behavior-change coaching can use SMART targets for refill timing, dose routines, symptom logs, and side-effect reporting thresholds.
Clinical Judgment Application
Clinical Scenario
A patient with newly diagnosed diabetes reports repeated unsuccessful attempts at diet and exercise change.
- Recognize Cues: Motivation exists but strategy is not sustainable.
- Analyze Cues: Prior plans were likely too broad and weakly measurable.
- Prioritize Hypotheses: A smaller, structured goal may improve adherence.
- Generate Solutions: Create one SMART nutrition goal and one activity goal.
- Take Action: Start plan with weekly check-ins and barrier review.
- Evaluate Outcomes: Confidence and consistency improve with measurable progress.
Related Concepts
- seven-pillars-of-self-care-framework - Domains where coaching goals can be applied.
- factors-affecting-adherence-and-compliance-in-patient-education - Motivation as a key adherence determinant.
- learning-readiness-and-teachable-moments-in-patient-education - Timing and readiness improve coaching effectiveness.
Self-Check
- How does intrinsic motivation change coaching strategy?
- Which SMART element is most often missing in failed plans?
- Why should goals be revised rather than abandoned after setbacks?