ANA Nursing Process Competencies
Key Points
- The ANA nursing process supports structured critical thinking and decision-making.
- Six competencies are assessment, diagnosis, expected outcomes, planning, implementation, and evaluation.
- These six competencies correspond to the ANA Standards of Practice used across settings and populations.
- In many bedside med-surg workflows, the same cycle is taught as five ADPIE steps, with expected-outcome identification embedded in planning.
- The framework is iterative and requires continuous reassessment and adjustment.
- Family and support-network participation can influence each step.
- ADOPIE is a practical mnemonic for the six ANA nursing-process steps.
- ANA standards apply to all RNs regardless of role, setting, specialty, or population.
- Consistent nursing-process use reduces omissions/duplication and supports collaborative, safer, more consistent care.
- ANA standards frame nursing practice as diagnosis and treatment of human responses to actual or potential health problems.
- Assessment competency requires the safest feasible assessment environment and respect for the patient as health decision-maker.
- Diagnosis competency includes risk/barrier identification, strengths recognition, patient-team verification, and documentation that supports collaborative outcome planning.
- Outcome identification is an RN function; LPN/VN roles center on awareness of outcomes and reporting response data within scope.
- Outcome-identification competency requires collaborative, evidence-based, culture/ethics-aligned outcomes with explicit attainment time frames.
- Planning is an RN function that prioritizes safety and uses standardized care-plan language; LPN/VN roles focus on implementation within scope.
- Implementation competency requires therapeutic, person-centered execution with evidence-based actions, interprofessional coordination, and accountable documentation of performed, modified, or omitted interventions.
- Evaluation is an RN function; LPN/VN may collect reassessment data, but the RN determines outcome status and care-plan revision.
- Evaluation competency requires criterion-based analysis against quality/safety standards with timely documentation, reporting, and transparent sharing of conclusions with the healthcare consumer and stakeholders.
- Evaluation is continuous during patient interaction, team discussion, and new lab/diagnostic review, and findings are documented in the medical record.
- Prioritization occurs in every ANA step: urgent cue focus in assessment, highest-risk diagnosis selection, safety-first planning, high-priority implementation, and outcome-focused evaluation.
- Reliable use of the nursing-process cycle is associated with more consistent care, fewer omissions/duplication events, and better patient satisfaction.
- The same process applies at community scale, where assessment and diagnosis target population trends and planning includes system/policy interventions.
Pathophysiology
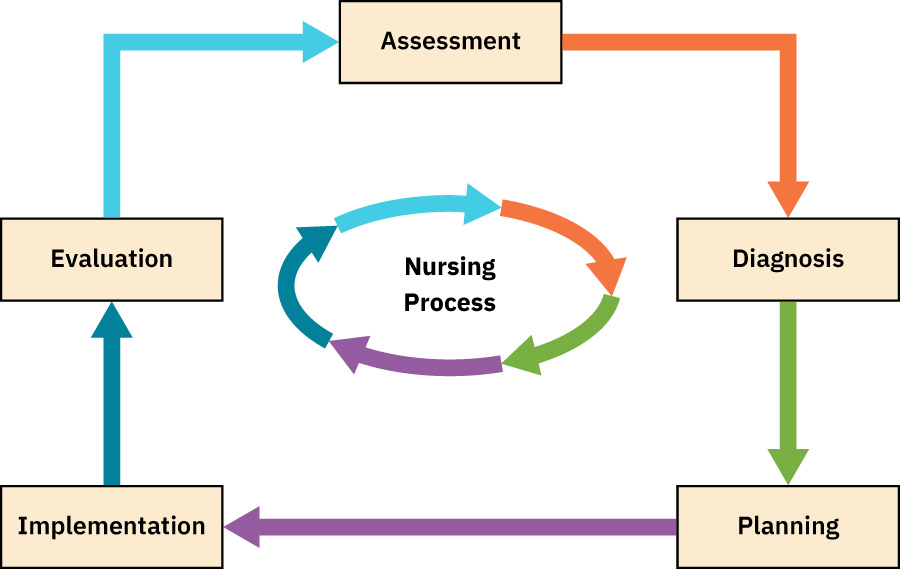 Illustration reference: OpenStax Clinical Nursing Skills Ch.1.
Illustration reference: OpenStax Clinical Nursing Skills Ch.1.
Patient status changes dynamically across disease progression and treatment response. A fixed one-time plan cannot safely account for new risks, partial response, or deterioration. The ANA competency sequence creates a repeatable loop that links data collection to action and outcome interpretation.
Classification
- Assessment: Gather and compare patient cues against expected norms.
- Assessment competency emphasis: Whole-person dignified data collection; culture/value/preference exploration; and communication-barrier identification including literacy, cognitive, financial, and sociocultural factors.
- Assessment forms: Focused assessments target a specific problem; comprehensive assessments establish broad baseline status and evolving whole-person needs.
- Assessment data workflow: Collect, validate across multiple inputs, organize by system/priority, and document clearly for team continuity.
- Diagnosis: Group cues into prioritized patient problems.
- Diagnosis competency emphasis: Identify actual/potential risks plus barriers (interpersonal, systemic, cultural, socioeconomic, environmental) and include patient strengths (support systems, health literacy, and self-care engagement).
- Diagnosis workflow: Identify potential concerns first, then refine to actual concerns and priority diagnoses before planning.
- Diagnosis toolset: Use standardized classification systems with technology and clinical decision-support tools, then verify diagnosis framing with the healthcare consumer and interprofessional colleagues.
- Outcome identification (expected outcomes): Set broad goals and specific measurable outcome statements before intervention planning.
- Outcome-identification competency emphasis: Co-define outcomes with the healthcare consumer and team, align with culture/values/ethics, derive from assessments/diagnoses, and support care coordination.
- Outcome timing and evidence standard: Integrate evidence/best practices, assign explicit attainment time frames, and document measurable goals for evaluation against safety/quality standards.
- Planning: Develop a collaborative, evidence-based, individualized strategy and prioritize interventions for safety and outcome attainment.
- Planning categories: Initial planning builds diagnosis-linked priorities/outcomes, ongoing planning revises or closes elements as conditions change, and discharge planning defines post-discharge supports/resources.
- Planning competency emphasis: Include implementation pathway details (timeline, steps, milestones), coordinate continuity of care, and account for cost/economic implications.
- Planning governance standard: Ensure plan compliance with statutes/rules/regulations/professional standards and document with standardized terminology.
- Implementation: Carry out planned interventions.
- Implementation competency emphasis: Use caring behaviors/therapeutic relationship, partner with the health care consumer for safe/effective/efficient/timely/equitable care, and coordinate with interprofessional partners across the continuum of care.
- Implementation delegation/accountability standard: Delegate using five-right factors (task, circumstance, person, communication, supervision/evaluation), align decisions with Nurse Practice Act/regulatory policy, and keep RN accountability explicit.
- Implementation documentation standard: Document interventions and any care-plan modification, including clinically justified changes and omissions.
- Evaluation: Determine whether outcomes are met, partially met, or unmet by the stated timeframe, then revise priorities and interventions as needed.
- Evaluation competency standard: Use applicable criteria frameworks (for example QSEN, Quadruple Aim, and IHI), evaluate against plan structure/process/timelines, and revise diagnoses/outcomes/plan/implementation as needed using ongoing data, benchmarks, and evidence synthesis.
- Evaluation reporting standard: Document results, report evaluation data in a timely manner, and share conclusions with the healthcare consumer/stakeholders for clarity and transparency per legal/organizational/professional requirements.
- Teaching-process alignment: The same six-step loop applies to learner assessment, educational diagnosis, teaching objectives, teaching-plan design, delivery, and learning evaluation.
- Stress-adaptation workflow mapping: Recognize risk-factor cues, analyze likely stressor(s), prioritize coping targets, generate constructive actions, take action, and evaluate whether adaptation improved.
- ADPIE bedside mapping: Many units operationalize this as assessment, diagnosis, planning, implementation, and evaluation, with expected outcomes documented in the planning step.
- Community-application mapping: At population level, ADPIE can structure community assessment, community diagnosis, intervention planning, implementation, and program evaluation cycles.
Nursing Assessment
NCLEX Focus
Evaluation is not the end; it is the trigger for the next assessment cycle.
- Collect objective and subjective data at baseline and after interventions.
- Create the safest possible setting for assessment and establish privacy/psychological safety before sensitive data collection.
- In stress-coping care plans, include acute/chronic stress cues, crisis signs, SDOH stressors, maladaptive-coping indicators, defense mechanisms, support-system quality, and caregiver-burden cues.
- In stress-adaptation assessment, include predisposing risk factors such as early-life adversity, prior coping history, outlook patterns, and chronic health/surgical sequelae that can lower coping reserve.
- Collect data using interviews, observation, physical examination, laboratory findings, and chart review.
- Recognize the healthcare consumer as the decision-maker and validate analysis directly with the patient whenever feasible.
- Combine free interview, focused prompts, and validated tools when assessing modifiable lifestyle behaviors (for example tobacco use, activity pattern, sleep pattern, and preventive-care status).
- Integrate local, regional, national, and global health-priority context when it changes risk interpretation or screening emphasis.
- Validate key findings by cross-checking patient report, family/caregiver input, team communication, and chart history when available.
- Organize findings by body system and immediate risk priority to support pattern recognition and hypothesis testing.
- Prioritize data collection by immediate condition and anticipated near-term needs.
- During assessment, capture urgent symptoms and instability cues first, then collect lower-acuity contextual data.
- Include physiologic, psychological, sociocultural, spiritual, economic, and lifestyle domains in assessment.
- Choose focused assessment when addressing one immediate concern, and comprehensive assessment when baseline or complex multidomain understanding is required.
- Prioritize problems by safety risk and progression potential.
- During diagnosis formulation, include barrier domains (interpersonal, system, cultural, socioeconomic, environmental) and strengths domains (support systems, health literacy, and self-care engagement).
- Validate diagnosis framing with the patient and interprofessional team before finalizing plan-critical priorities.
- Document assessment findings in a clear, concise, and accurate format because documentation is both a legal record and a care-coordination tool.
- Build a broad goal first, then specific expected outcomes that describe measurable client actions.
- Match short-term and long-term goal horizons to care setting and acuity (for example shift-level in critical care vs monthly horizons in outpatient care).
- Ensure expected outcomes are measurable and time-bounded.
- Construct expected outcomes in explicit SMART format: specific, measurable, attainable/action-oriented, realistic/relevant, and time-limited.
- Start outcome statements with
The client will..., keep one action per statement, and align wording to defining characteristics of the nursing diagnosis. - Confirm the outcome target is realistic for the current context and that the client is willing to participate in achieving it.
- Prefer objective indicators and measurable verbs; avoid vague terms like
normaloradequatewithout a numeric or observable target. - Replace imprecise phrases (for example,
once in a while) with explicit measurable targets (for example,once per week) before finalizing outcomes. - Keep planning documentation in standardized care-plan terminology to preserve continuity across shifts and disciplines.
- Track whether interventions are feasible for patient and support network.
- Reassess quickly when outcomes are partially met or unmet.
- During evaluation, classify each expected outcome as met, partially met, or unmet by its target timeframe.
- Use criterion-based evaluation (quality/safety/effectiveness/efficiency/timeliness/equity) when judging outcomes and revising strategies.
- Compare actual outcomes with expected outcomes against safety and quality standards, then modify outcome targets when condition/status changes.
- Trigger reassessment during patient interaction, interprofessional care-plan discussion, and review of updated labs/diagnostics.
- Account for technology-enabled assessment changes (for example telehealth and AI-assisted workflows) while preserving RN judgment and data validation.
- Recognize and mitigate personal attitudes, values, and bias that can distort assessment interpretation.
- Keep RN responsibility explicit for data analysis, diagnosis, and outcome identification; LPN/VN support data collection within scope but do not perform diagnostic analysis.
- Keep RN responsibility explicit for initial physical exam and interpretation; follow-up exam elements (including selected vitals/weight collection) may be delegated per policy with RN supervision and documentation oversight.
- Use ABCs/Maslow and time-sensitive consequence logic during implementation prioritization, with least invasive effective options preferred when clinically appropriate.
Nursing Interventions
- Build care plans with explicit links between diagnosis, intervention, and expected outcomes.
- Maintain RN accountability for creation and revision of the nursing care plan.
- Keep plans individualized to the patient even when standardized templates are used for workflow efficiency.
- Build compassionate, appropriate intervention choices that minimize unwanted treatment burden and unnecessary suffering while preserving safety.
- Build diagnosis-to-plan transitions by separating potential concerns from confirmed current concerns before selecting interventions.
- In stress-adaptation plans, explicitly separate constructive actions (resource-access and coping-supportive) from destructive actions (secondary distress-generating) before implementation.
- Engage patients and caregivers in goal-setting so outcomes reflect client values, culture, and desired priorities.
- Identify barriers to realistic outcome attainment (for example pain, mobility limits, health-literacy gaps, or resource constraints) and revise targets early.
- Use focused anxiety-reduction strategies (calm approach, procedural explanation, cue control, and coping-skill coaching) when stress impairs participation.
- For coping-enhancement implementation, establish a calm/accepting low-stimulus environment and prioritize immediate safety modification plus provider notification when self-harm intent is identified.
- Escalate collaborative needs when independent nursing scope is insufficient.
- Review concerning laboratory/diagnostic findings with the provider and verify prescription appropriateness before implementation when status has changed.
- Modify interventions when evaluation shows limited effectiveness.
- If outcomes are partially met or unmet, reassess diagnosis accuracy, outcome realism/timeframes, barriers, and intervention fit before revising the plan.
- Continue iterative cycles until goals are achieved or revised.
- Delegate selected implementation tasks to LPN/VN or trained UAP only when scope/policy criteria are met and RN supervision is available.
- When delegating, confirm five-right conditions and Nurse Practice Act/regulatory-policy alignment before task transfer.
- Coordinate implementation through collaboration and communication across care settings, including transition points.
- Include care coordination and health teaching/health-promotion actions within implementation planning.
- Begin discharge-planning elements early and update them during ongoing planning so transition needs are resolved before discharge.
- Contribute to continuous improvement of planning systems at unit/organization level when recurring plan-design barriers are identified.
- If reassessment shows a planned intervention is unsafe, hold the action, document rationale, notify provider, and communicate the change during handoff.
- Document performed interventions and any modification/omission of planned actions in the medical record with rationale.
- Document evaluation conclusions and resulting care-plan revisions in the medical record.
- Report and share evaluation data/conclusions with the patient and involved stakeholders in a timely, transparent manner.
- Maintain current care-plan documentation to meet organizational and regulatory expectations for coordinated, individualized care.
Loop Failure Risk
Skipping evaluation or failing to revise an ineffective plan increases risk of prolonged instability.
Pharmacology
Medication-related interventions should be evaluated with the same loop: indication, response, adverse effects, adherence barriers, and plan adjustment.
Clinical Judgment Application
Clinical Scenario
A patient with multiple diagnoses shows partial improvement after initial care plan implementation.
- Recognize Cues: Some outcomes improving, others stagnant.
- Analyze Cues: Current plan is only partially effective.
- Prioritize Hypotheses: Unmet outcomes may require revised interventions.
- Generate Solutions: Update priorities and intervention set.
- Take Action: Implement revised plan with clearer metrics.
- Evaluate Outcomes: Determine whether revised strategy produces full progress.
Related Concepts
- categories-of-nursing-diagnosis - Diagnosis category choice informs planning strategy.
- nursing-diagnosis-vs-medical-diagnosis - Clarifies diagnosis focus used in competency steps.
- evaluation-of-outcomes-in-fluid-electrolyte-and-acid-base-care - Practical example of the evaluation-revision cycle.
Self-Check
- Why must expected outcomes be defined before intervention selection?
- What should happen when a plan is only partially effective?
- How does support-network involvement alter implementation and evaluation?